Occupational well-being is how you use your skills and abilities to enrich your own life as well as the lives of those around you. Attitude is related to satisfaction regarding your work, whether it be paid or unpaid.
The purpose of this pilot study was to evaluate the effect of a web-based education module on the knowledge, attitudes, and ratings of willingness to access help related to suicide prevention in psychiatric-mental health nurses.
Congratulations to Michele Van Outer, DNP, BSN, on her graduation from the University of Kentucky (UK) College of Nursing (CON) with her Doctor of Nursing Practice (DNP). Dr. Van Outer’s project, “Improving Structural Empowerment Through the Co-Creation of a Professional Governance Program of Nurse Managers and Frontline Nurse Leaders” aims to uncover the potential benefits of a collaborative approach on staff members’ patient care outcomes. Dr. Van Outer serves as a Nurse Manager at Eastern State Hospital (ESH).
Dr. Van Outer began her career as an associate degree Nurse (ADN) at ESH developing her skill in patient care. Over time, she completed her BSN and is graduating May 2024 with her DNP in the Executive Leadership track. From her time as a floor nurse to her DNP, Van Outer has consistently found herself in leadership roles where she can impact best practices for patient care.
Dr. Van Outer has always been passionate about community support and public health relations and how they impact patient care. During her early nursing education, she was already interested in mental health and psychiatric nursing. She understands how inpatient psychiatric hospitals provide crucial support for underserved communities, often serving as a last resort for seeking care. Dr. Van Outer states, “We provide evidence-based care at ESH for people who, maybe, wouldn't be able to access it any other way.”
Throughout her academic journey, Dr. Van Outer mentioned how beneficial the support was from her cohort and the Work Learning Program (WLP) at ESH. She specifically appreciated Dr. Okoli’s writing workshops and the support from WLP leaders in reviewing papers and conceptualizing assignments. She notes, “It was a four-year program; so, with that extra support, it enabled us to keep going because when you got in a bind, we had each other, but we also had the Work Learning Program (WLP) and their experience and research.”
Dr. Marc Woods, Chief Nursing Officer with UK Health Care notes, "Dr. Michelle Van Outer's resilient pursuit of her doctoral degree showcases her unwavering dedication to leadership in nursing. Her work on shared governance not only enhances her capabilities but also inspires others in the healthcare field to excel in this area."
Now that Dr. Van Outer has successfully completed the DNP program, she has time to appreciate her new accomplishment. Her goal remains to eventually transition into a director position and to continue to support nurse leaders.
People living with serious mental illnesses (SMI) continue to face a disproportionate burden of tobacco-related prevalence, morbidity, and mortality as compared to those without SMI. The risk of mortality related to cigarette smoking among those with SMI is six-times that for persons without SMI.
The authors regret the following error. The second affiliation of the first author was omitted from the article. The corrected affiliations are as follows:
State Key Laboratory of Oral Diseases & National Center for Stomatology & National Clinical Research Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan, China;
School of Nursing, Chengdu University of Traditional Chinese Medicine, No. 1166 Liutai Road, Wenjiang District, Chengdu City, Sichuan province 611137, China.
We have all likely experienced the shame, pain, and sting of being stigmatized at some point. Stigmatization appears in diverse forms-including derogatory comments about skin tone, hair texture, or body size; denial of resources due to social standing; and devaluation of persons because of sexual/gender identity, religious affiliation, or political preferences. Regardless of its form, stigmatization is never productive and poses a considerable threat to mental health and well-being.
In the world of Social Work, there are many frameworks and theories that professionals use with clients in their treatment plan. The change process, developed by Prochaska and DiClemente in the late 1970s, is a model that allows healthcare professionals to meet the client where they are in their readiness to change. This is essential for supporting behavioral health clients as they work toward change. Identifying where a client is in their readiness to change allows the social worker and client to work together to select an intervention that is most appropriate for the client’s readiness to change. Social workers use this model understanding that change is not necessarily a linear process, as clients move along the continuum. This model can be applied in any social work setting to support clients and promote their autonomy so that they are able to move forward at their own pace.
Pre-Contemplation
In this stage, the client does not have the intention to change. They are not aware that their behavior is creating a challenge for themselves. They may choose to defend their current behaviors when others ask if they are interested in change. For example, a client who smokes one pack of cigarettes a day may express frustration with friends and family who are concerned about their tobacco use and its health effects.
Pre-Contemplation Example
Social worker: “Thank you for sharing that you are using tobacco. Are you interested in stopping tobacco use?”
Client: “I enjoy using tobacco, especially with my friends. I don’t want to talk about it today.”
Contemplation
During contemplation, clients know they are experiencing a challenge and are considering a change in their behavior. However, they are not fully committed to change. This stage may include weighing the pros and cons of change, identifying barriers to change, and experiencing conflicting emotions. Clients may remain in the contemplation stage for prolonged periods of time. For example, a client who smokes one pack of cigarettes a day may begin to consider stopping tobacco use, make a list of pros and cons, but not be quite ready to start the process of stopping.
Contemplation Example
Client: “Maybe I do need to change. But, I don’t know that I’m ready.”
Social worker: “So, you understand that change is important but maybe you are not quite ready to change.”
Preparation
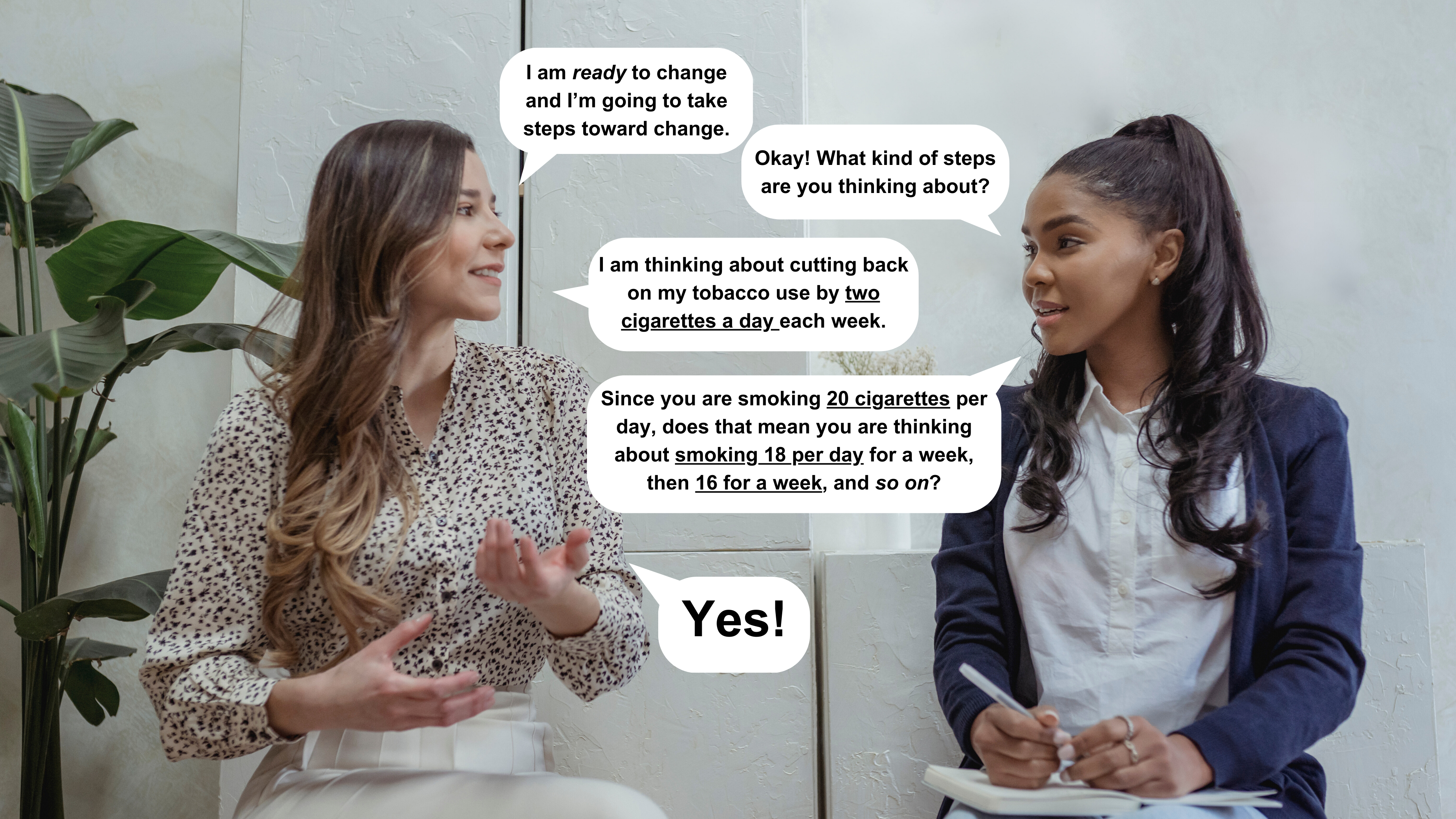
This stage is when a client is ready to take steps toward change, usually within the next month. The client will begin to experiment with small changes and may make a list of goals, prepare an action plan, or collect information about the change they wish to make. For example, if a client’s goal is to stop tobacco use, they may take steps such as smoking less each day or learning about the health benefits they will experience after quitting.
Preparation Example
Client: “I am ready to change and I’m going to take steps toward change.”
Social worker: “Okay! What kind of steps are you thinking about?”
Client: “I am thinking about cutting back on my tobacco use by two cigarettes a day each week.”
Social worker: “Since you are smoking 20 cigarettes per day, does that mean you are thinking about smoking 18 per day for a week, then 16 for a week, and so on?”
Client: “Yes!"
Action
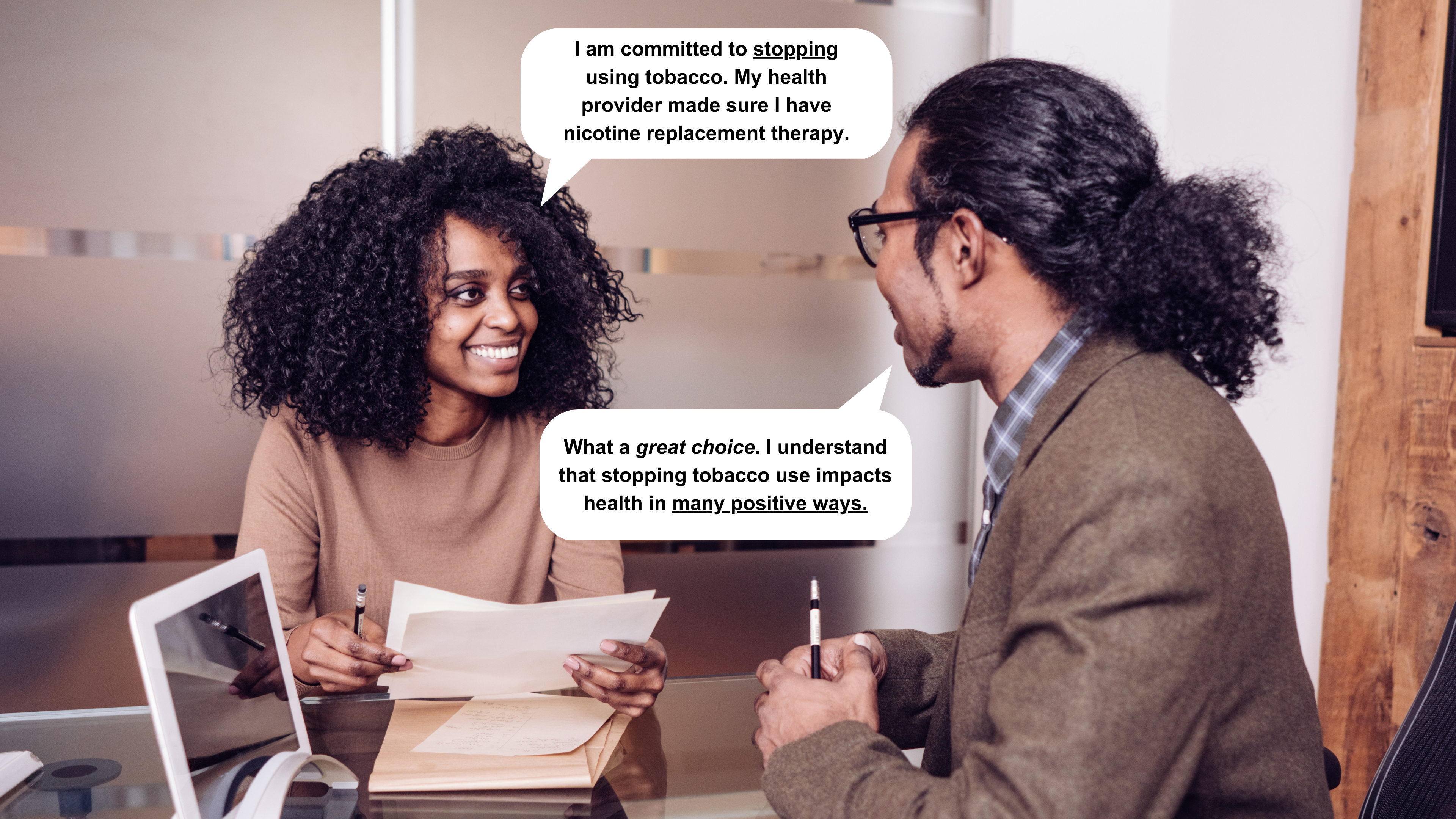
The action stage is characterized by behavior modification and action toward a goal. The client is changing the behavior or aspect of their life that has created a challenge. In this stage, support from family and friends is important as a client works toward change.
Action Example
Client: “I am committed to stopping using tobacco. My health provider made sure I have nicotine replacement therapy.”
Social worker: “What a great choice. I understand that stopping tobacco use impacts health in many positive ways.”
Maintenance
In the maintenance stage, the client will avoid former adverse behaviors, maintain healthy coping mechanisms, and stay focused on their goals and recovery. They may continue counseling, support groups, and interacting with an accountability partner. People committed to maintaining change can do so for their entire lives.
Maintenance Example
Client: “I’m so proud of myself. I stopped using tobacco 3 months ago. My accountability partner, counseling, and support group have been a huge help.”
Social worker: “I’m so proud of you.”
Clients can be in different stages of the change process in different areas of their life. For example, a client may be in the pre-contemplation stage in relation to their readiness to stop using alcohol. This same client may be in the action phase in relation to stopping tobacco use.
BH WELL exists to promote behavioral health and wellness among individuals facing behavioral health challenges. Learn more about BH WELL at https://bhwell.uky.edu. Follow us on social media.
Why should you care about the health and well-being of your legislators?
The legislative session is in full swing in Kentucky. The schedules senators and representatives keep during this time are long and the issues discussed may impact you personally. Could your legislator’s occupational balance affect you? Try applying the seven domains of occupational science to legislator as an occupation and see!
Activities of Daily Living and Instrumental Activities of Daily Living
Activities of Daily Living (ADLs) are basic tasks that people do daily such as bathe, manage personal hygiene and eat. Everyone, including legislators, function best when ADLs are met. Beyond these essential and routine ADL tasks, there are Instrumental Activities of Daily Living (IADLs). These tasks include managing finances and clearly communicating ideas. Given that legislators are responsible for making decisions about how our taxes are spent and what bills become laws, a legislator’s level of advanced thinking is essential so they can best serve you and your community.
Health Management
Taking care of one’s health, eating well-balanced meals regularly, and allowing breaks to recharge during stressful days are all necessary to maintain good health. Managing health is one way a legislator can assure they will be present more, absent less, and better able to serve you.
If a legislator has health issues, they may miss work or fall behind in their work priorities. For a legislator, this could mean being absent for a critical vote. If an issue you feel strongly about is up for a vote, but your legislator is home sick, they will not be able to vote on that particular issue even if you have communicated effectively with them.
Rest and Sleep
Several legislators have been “caught” on camera falling asleep during session over the years. If your legislator is tired during session, they may miss important discussions taking place on the floor. These discussions involve potential bills that could become laws on a broad array of issues from education to health to taxes. Decisions made on issues impact everyone. Given that they are in a high-stress environment and career, legislators need adequate rest to process information quickly and effectively. Might there be a day when your legislator needs to rest or nap in their offices between meetings? Yes! Adapting sleep patterns in this way allows them to be alert during the most critical times.
Education and Work
Have you ever thought about how much information your legislator must learn? Legislators must understand how to draft a bill, find co-sponsors, discuss, and promote issues that are of high importance to their communities, and more. There is much to learn so that the work can begin.
Beyond the legislative process, community members expect legislators to be up-to-date on a wide variety of issues. You need your legislators to read, listen and learn about new topics in a critical way that values best practices and evidence-based science.
Work for your legislator does not end when the day’s meetings conclude. Legislators often volunteer alongside those who voted them into office. This gives you opportunities to participate in these local experiences and get to know your legislator. Imagine talking to your legislator about issues that are important to you! You can have those conversations by seeing them in your hometown or by visiting their office.
Leisure
Sometimes you may see your legislator playing golf or going to a sporting event and you may question why they are spending time engaging in leisure activities during a legislative session. Participating in such activities helps your legislator avoid burnout. They can return to their next day’s session refreshed and better ready to serve you.
Social Participation
Most legislators enjoy activities in their own communities. Beyond that, local events allow legislators to discuss issues with you during re-election campaigns. Legislators are there to represent their constituents. Sometimes you and your legislator will see an issue similarly and sometimes you will see it differently. Allowing your legislator the opportunity to know you on a more personal level will help them understand why certain issues are important to you.
As you can see, there are many reasons why it serves you better if your legislator has occupational balance. Through the lens of Occupational Therapy, a legislative career may create barriers to occupational balance, requiring dedication to bring these seven domains back into working order, especially during a legislative session.
I asked a new Kentucky legislator, Amanda Mays-Bledsoe, if she found the balance to be a challenge and, if so, which of the seven domains she has found to be most challenging during this legislative session. Senator Mays-Bledsoe replied, “A mentor told me that, in the beginning, it’s all overwhelmingly new – the people, the physical location, the protocol of session, the legislation, the intense schedule not to mention the fast pace. Only experience will help build muscle memory to allow for more margin. I’m trying to balance learning it all while maintaining the understanding that it’s going to take time. I am fortunate to come home at night to see the kids but session is mentally, physically, and emotionally exhausting leaving little to give them. The phone calls and e-mails come in high volume about bills with little time to respond. Sleep has been challenging as the conversations and material from the day continue to replay in my head. No question, this is one of the harder things I’ve done. Even so, I’m committed to keep learning and trusting that I will be a stronger legislator and person in the end.”
And in finding that balance, occupational science confirms that a legislator will be stronger and make better decisions for you, the ones who voted for them!
...
Occupational therapy is a health-based profession that uses physical and social-emotional considerations to provide quality of life, and health and well-being to our clients. Using skills to enhance everyday living makes occupational therapists unique among the healthcare team.
The University of Kentucky Behavioral Health Wellness Environments for Living and Learning (BH WELL) research team works to promote behavioral health and wellness among individuals facing behavioral health challenges. Mental health is health.
Resources
American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010. https://doi.org/10.5014/ajot.2020.74S2001
Battaglini, M., Sciabolazza, V. L., & Patacchini, E. (2018). Effectiveness of connected legislators. American Journal of Political Science, 64(4). https://doi.org/10.3386/w24442
For hundreds of years, there has been a dynamic duo in the hospital setting: the social worker and nurse. A healthy partnership between social workers and nurses is vital as they both provide effective, holistic care. Here are 7 key elements of the partnership between social workers and nurses that contribute to positive patient outcomes:
1. Partnering in Patient-Centered Ethical Duties
In the National Association of Social Workers (NASW) Code of Ethics (1996), social workers are ethically bound to support the dignity and worth of a patient. In the same way, the American Nursing Association (ANA) Code of Ethics (2015) calls for nurses to protect human dignity and patient rights. Each profession’s training requires a patient-centered focus.
2. Assessing a Patient’s Physical and Psychological Needs
Identifying needs and desires of a patient is one of the first steps of the social work and nursing team. As part of a multidisciplinary team, social workers and nurses contribute to the development of each patient’s treatment plan. The nurse will assess a patient’s medical and psychological needs and provide care to ensure that these needs are met according to their professional scope and standards, clinical guidelines, and best practices. Social workers also complete an evidence-based biopsychosocial assessment early in treatment to inform a patient’s individual treatment plan. This assessment serves as a guideline in discharge planning, where the social worker determines the various environmental, social, medical, and family supports that a patient will need upon discharge.
3. Advocating for Patient’s Autonomy and Rights
Social workers and nurses each play key roles to ensure that every part of a patient’s treatment is ethical, appropriate, and respectful. Both social workers and nurses remain aware of any barriers throughout a patient’s treatment, initiating investigations for abuse and neglect (as needed), informing a patient of their treatment options during care, maintaining confidentiality, and including them in all decisions regarding their treatment.
4. Answering Questions for a Patient or their Family
With a multitude of factors which require consideration in a patient’s treatment, it is natural for a patient and family to have questions concerning timeline, the treatment plan, medications, and long-term care. In this dynamic duo, nurses take the lead on conversations concerning a patient’s diagnosis, treatments, and medication management. In turn, the social worker takes the lead on conversations about long-term care plans, providing counseling in challenging situations, and connecting the family to needed resources. As such a dynamic duo, both the social worker and nurse ease a patient and their family’s minds, which can lead to better health outcomes. In fact, when patients are educated about their diagnosis and treatment plan better health outcomes can be expected (Fernsler, J. I. et al, 1991).
5. Individual and Group Counseling
Diagnosis and treatment plans can be challenging for patients and families. Making lifestyle changes to improve wellness can often seem overwhelming. A nurse's rapport with a family can create opportunities to offer emotional support and referral to a social worker if needed. A social worker may counsel patients and families individually to process these feelings and challenges in behaviors and skills to achieve recovery. In addition, patients and families may participate in group counseling sessions. Group counseling is an evidence-based practice that allows individuals to receive treatment together in a group with others who may be experiencing similar life stressors.
6. Providing Financial Planning and Assistance
In addition to concern for their loved ones, families frequently endure financial stress related to healthcare and hospital stays. While the nursing team works to ensure proper medical treatment and recovery, the social work team is tasked behind the scenes to address the financial situation with the family. As recovery is underway, social workers may refer patients to legal aid, federal financial assistance programs, community-based resources, and payment plans provided by the healthcare institution.
7. Developing Discharge Plans
Nurses and social workers alike are proponents of a patient living their best life after hospitalization. However, the social worker and nurse assist a patient and family leading up to discharge in different ways. The nurse will provide timely communication with a patient and family regarding medical assessments and ongoing care needs. This includes explaining to a patient and family regarding all necessary health information, medications, and other health needs. In a complimentary manner, the social worker’s role for discharge planning focuses on securing housing (or other accommodation) placement, financial resources, and social support. The social worker may coordinate ongoing patient and family assessment and counseling, follow-up, and community resources needed to ensure continuity of care after discharge.
Conclusion
The collaboration between social workers and nurses in hospital settings creates a dynamic duo. Together, they have the common goal of providing care to patients in ways that enhance patient outcomes. Partnering in ethical duties, assessing patients’ physical and psychological needs, advocating for patients’ rights, providing individual and group counseling, financial planning and assistance, and developing discharge plans are all ways that social workers and nurses work together toward providing excellent care.
References
Code of Ethics for Nurses. American Nurses Association. (2017, October 26). Retrieved November 17, 2022, from https://www.nursingworld.org/practice-policy/nursing-excellence/ethics/code-of-ethics-for-nurses/
Fernsler, J. I., & Cannon, C. A. (1991). The whys of patient education. Seminars in oncology nursing, 7(2), 79–86.
National Association of Social Workers. (1996). Code of ethics of the National Association of
Social Workers. NASW Press.
Social Workers in healthcare: How they make A difference. Adelphi University Online. (2021, June 10). Retrieved May 18, 2022, from https://online.adelphi.edu/articles/social-workers-in-healthcare-how-they-make-a-difference/
Williams, C. C., Bracht, N. F., Williams, R. A., & Evans, R. L. (1978). Social work and nursing in hospital settings: a study of interprofessional experiences. Social work in health care, 3(3), 311–322.
We examined demographic, work-related, and behavioral factors associated with witnessing and/or experiencing workplace violence among healthcare workers.
Prior to the beginning of the century, very little literature existed that discussed the impact of architecture on mental and behavioral health recovery. As a result of this, a larger emphasis has been placed upon conducting research that reveals the true intersection of architecture with mental health care, and how it contributes to positive mental health outcomes.
An interdisciplinary team of researchers at the University of South Australia found that there had been an increase in academic interest in the relationship between mental health care and architecture at the turn of the century, particularly between 2008 and 2013. Many key themes have been identified across published literature relating architecture to mental health care. The three prominent themes include security, light, and the impact of architecture on health outcomes. This blog provides examples of each of these themes through the use of photos from Eastern State Hospital’s old and new facilities. These photos provide examples of exactly how far architecture has come in playing a key role in behavioral health inpatient care and recovery.
Security
Security is very important to mental healthcare facilities. As reported by a Haller and Deluty study in 1988, psychiatric hospitals and units in the U.S. have a significantly higher average number of assaults per bed yearly than non-psychiatric hospitals or units. As such, it is extremely important for architects to design mental healthcare facilities that allow these issues to be quickly resolved. In a mental healthcare facility, security includes the ability to effectively and swiftly respond to acts of aggression from inpatients and to mitigate the impact of environmental stress on patients and staff alike.
The safety of patients and staff are at the forefront of every design decision. The new facilities at the Eastern State Hospital campus, located in Lexington, Kentucky, are a testament to the careful planning and execution of safety both during the architectural design and construction phases. The architecture was designed to support a secure, safe environment for serving inpatients and conducting daily operations. Emphasis is also placed upon what is referred to by Jayaram and Herzog as “SAFE MD”:
S- Suicide
A- Aggressive behavior and promotion of the safe use of seclusion and restraints
F- Falls
E- Elopement
M- Complications when dealing with medical comorbidities
D- Drug / Medication errors
This is an area where the impact of architecture on mental health is extremely apparent. Here are two examples of how Eastern State Hospital’s new facility better provides safety according to the SAFE MD areas of concern:
S- Suicide
The old hospital had complete doors in patient rooms, regular door handles, and other features that would not give way if a patient were trying to cut off their breathing pathway. The new hospital features doors with triangle cutaways, door cuffs instead of handles, and other features that enhance safety and reduce the likelihood of suicide attempts.
Note how the bed and the windows of the old hospital bedrooms make it more difficult to create an environment free of pathways to suicide such as bars on the beds and open windows.
The new hospital has beds, doors, and windows designed to create a safe environment for those contemplating suicide.
E- Elopement
The old hospital was disjointed and had numerous doors from which entry/exit could occur, increasing the likelihood of elopement. While still meeting or exceeding the fire code, the new hospital has fewer entries for each unit and only three entry/exit points into the hospital.
The original ESH built in 1817
The new facility was built with numerous windows and courtyards.
Light
Light and lighting is the second category that impacts patient recovery. Spaces that have special meaning to patients can be made to stand out and can be defined with emotive lighting and colors. Lack of natural light is linked to many issues in published literature, including eating disorders, depression, circadian rhythm disruptions, and poor sensory stimulation. Since light affects mood and perception, it is important for mental health recovery. Architecture can design spaces with adequate natural and artificial lighting. This can include features such as the placement of rooms in relation to the rotation of the sun, and the inclusion of enough windows to allow adequate natural light into the space.
In the photos above, notice that the windows were smaller in the old hospital. In fact, some rooms that housed several patients only had one small window. In contrast, the new hospital allows every patient to have a room with a view, also shown in the photos above. It also provides a sunroom and even an outdoor courtyard for soaking in the sun. The new hospital is Silver LEED-certified, in part because of how well it incorporates light. Achieving Silver LEED certification requires much hard work and dedication during the planning, design, architectural, and construction phases to assure that a supportive, sustainable environment exists.
A bedroom for multiple patients with little natural light in the old facility.
A day room with large windows allowing increased natural light.
The Impact of Architecture on Health Outcomes
The impact of architecture on health outcomes is primarily focused on aesthetics and sensory stimulation, which is directly related to the spatial design of a mental healthcare facility. Spatial design is when the designer thinks about how the space feels, is organized, and might feel to the person experiencing the environment. Architecture plays an important role in creating an environment that directly impacts stress levels and social interactions. For a behavioral health facility such as Eastern State Hospital, there needs to be a balance between what is best for the patients, how the community perceives the design, and how all health and building regulations are met. Creative conflicts may arise when attempting to meet these environmental requirements, thus creating an issue that may prevent the “perfect” patient facility from existing. For example, the need for patients to have access to health professionals can be in opposition to the need for health professionals to have separate areas for medication preparation, charting, and behavioral health team discussions. The compromise made at Eastern State Hospital shows the huge contrast between the old hospital nurse stations and the new open team stations with private areas incorporated into the design as well as full glass walls in the dayroom allowing for easy patient observation while still allowing the patients a sense of privacy.
The former nursing station.
A nursing station in the new facility.
ESH is a 239-bed inpatient psychiatric hospital located in Lexington, Kentucky. They are the oldest continuously operating psychiatric hospital in Kentucky and the United States, having provided care to individuals requiring mental and behavioral health inpatient services since 1824.
Hunter McKenzie worked as a BH WELL project assistant until he graduated from the University of Kentucky College of Design in 2021 with a Bachelor's degree in Architecture and is now working toward his Masters of Architecture at Columbia University.