Social well-being is the ability to interact in a healthy way with those around us. This involves having supportive friends and family, developing deep connections, and the ability to communicate in healthy ways.
Partner Spotlight: Green River District Health Department
The Green River District Health Department (GRDHD) is located in Western Kentucky and serves seven counties – Daviess, Hancock, Henderson, McLean, Ohio, Union, and Webster. GRDHD’s mission is to “promote, protect and strengthen the health and well-being of all by helping develop and maintain healthy lifestyles and environmentally safe communities.” Since 1998, GRDHD has been working to educate the community about the dangers of tobacco use and secondhand smoke exposure through its tobacco prevention and education program. As part of their partnership with the Behavioral Health Wellness Environments for Living and Learning (BH WELL) research team, GRDHD supports behavioral health organizations working towards advancing tobacco-free policy and tobacco treatment services for people living with mental or behavioral health challenges who want to stop tobacco use.
People living with a mental or behavioral health challenge who use tobacco have a substantially reduced life expectancy and may die 10-25 years earlier than those who do not have a mental or behavioral health challenge and do not use tobacco. The most common causes of death among people living with mental and behavioral health challenges are heart disease, cancer, and lung disease, all of which can be caused by tobacco use. Provision of tobacco treatment services has a positive impact on both the mental and physical health outcomes of people living with mental and behavioral health challenges and can aid in recovery. Given such an impact, GRDHD works diligently in the community to integrate tobacco treatment services within local mental and behavioral health organizations.
Gary Hall, GRDHD Health Educator II, leads the tobacco prevention and education program at the health department. He assists behavioral health organizations working towards tobacco policy and tobacco treatment integration. Prior to his position with GRDHD, Hall spent 27 years with RiverValley Behavioral Health (RVBH), where he served in many roles including Director of RVBH’s Regional Prevention Center. In 2023, Hall received the David B. Stevens, MD, Smoke-free Advocate of the Year Award, one of the most prestigious honors awarded by the Kentucky Center for Smoke-free Policy. Hall’s expertise in behavioral health and tobacco prevention allowed GRDHD to support RVBH as they implemented a tobacco-free policy and integrated tobacco treatment system-wide in 2023. RVBH shares that, "Gary has been such a valuable resource to our team at RiverValley Behavioral Health while developing and implementing our smoke-free policy. His commitment to health and wellness is not only focused on our community mental health center but for the entire population in the Green River district. Gary served as a consistent collaborator to our team by sending us resources, data and relevant information related to NRT to guide our conversations, workplan and policy. He is a champion in the field and we are grateful to have him as a colleague".
This tremendous collaborative effort was recognized by BH WELL in the fall of 2023 when RVBH was presented with the 2023 BH WELL Tobacco Treatment Integration Award. BH WELL Director Dr. Zim Okoli celebrated their accomplishment and shared that, "Although the stigmatization of people living with mental and behavioral health challenges has normalized tobacco use in mental and behavioral health settings, community partners like Green River District Health Department and RiverValley Behavioral Health are working hard to support mental health and recovery by normalizing tobacco-free environments and access to tobacco treatment services.” Increasing accessibility and availability are two essential ways to break down disparities in tobacco use and the related health problems within the behavioral health community.
In addition to RVBH, GRDHD partners with many other community-based organizations as well as federal, state, and local government agencies. Hall believes one advantage of partnerships in the Green River District is the ease with which smaller community organizations collaborate. Each partner has a role to play in the successful implementation of tobacco-free policy and tobacco treatment service integration. There can be an impactful domino effect when one partner’s successes turn into another partner’s motivation toward these same goals.
Reflecting on his partnership with BH WELL, Hall shared, “Along with being patient, BH WELL reminded me about best practices. They provided research that we were not familiar with, especially regarding treatment success for individuals. In particular, they helped us understand comprehensive smoke-free policy, such as ensuring that it is campus-wide. BH WELL has acted as a guide for both RiverValley and the health department. I really believe if they hadn’t been a part of this, the progress wouldn’t look how it does today.”
Following best practices is what led RVBH to successfully implement its comprehensive smoke-free policy on August 1, 2023. For GRDHD, the most rewarding part of collaborating with RVBH on this effort was having the ability to impact change. Hall believes that this success would not have happened without federal and state tobacco control funding targeted toward the mental and behavioral health population. GRDHD receives funding from the Kentucky Tobacco Prevention and Cessation Program through a grant from the Centers for Disease Prevention and Control (CDC) specifically to support this type of work.
GRDHD Health Educators Gary Hall and Ethan Martin with Owensboro Health’s Holly Logsdon, RN, TTS, participating at the 2023 Kentucky Tobacco Control Conference.
GRDHD continues to promote tobacco treatment as a component of support for people working towards recovery from mental and behavioral health challenges. The team has many important projects on the horizon including a collaboration with an all-women's addiction recovery group where they plan to incorporate tobacco treatment services.
Collaborations such as this change lives. For example, Hall recalls BH WELL visiting RVBH with him to discuss going tobacco-free. In that meeting were several people who had been using tobacco but have now stopped. “This just shows the power of the conversation,” said Hall. To see this power in action, you can watch Mary’s story on stopping tobacco use here.
In this paper we aimed to explore: (1) challenges that people with mental illnesses (MIs) describe in engaging in smoking cessation, (2) challenges that mental health providers (MHPs) perceive that people living with MIs face, and (3) how the perceived challenges are similar and/or different from both perspectives. Semi-structured interviews were used to obtain narrative data from 16 MHPs and 13 psychiatric inpatients with MIs. We identified themes purport societal, group, and individual factors may influence smoking cessation treatment engagement. The scope of the perceived challenges appeared varied in the narratives of MHPs as compared to those with MI.
For this video, I am going to share with you common myths about mental health challenges and facts based on research that addresses these misconceptions.
1. Amer MM, Hovey JD. Anxiety and depression in a post-September 11 sample of Arabs in the USA. Social psychiatry and psychiatric epidemiology. 2012;47(3):409-418.
3. Wang PS, Berglund PA, Olfson M, Kessler RC. Delays in initial treatment contact after first onset of a mental disorder. Health Services Research. 2004;39(2):393-416.
4. Hasan AA, Musleh M. Barriers to seeking early psychiatric treatment amongst first-episode psychosis patients: A qualitative study. Issues in Mental Health Nursing. 2017;38(8):669-677.
5. Zolezzi M, Alamri M, Shaar S, Rainkie D. Stigma associated with mental illness and its treatment in the Arab culture: A systematic review. International Journal of Social Psychiatry. 2018;64(6):597-609.
6. Weatherhead S, Daiches A. Muslim views on mental health and psychotherapy. Psychology and Psychotherapy: Theory, Research and Practice. 2010;83(1):75-89.
8. Alhomaizi D, Alsaidi S, Moalie A, Muradwij N, Borba CP, Lincoln AK. An Exploration of the Help-Seeking Behaviors of Arab-Muslims in the US: A Socio-ecological Approach. Journal of Muslim Mental Health. 2018;12(1)
9. Aldalaykeh M, Al-Hammouri MM, Rababah J. Predictors of mental health services help-seeking behavior among university students. Cogent Psychology. 2019;6(1):1660520.
10. Rice AN, Harris SC. Issues of cultural competence in mental health care. Journal of the American Pharmacists Association. 2021;61(1):e65-e68.
11. Eldeeb SY. Understanding and Addressing Arab-American Mental Health Disparities. Scholarly Undergraduate Research Journal at Clark. 2017;3(1):1.
12. Arboleda-Flórez J, Stuart H. From sin to science: fighting the stigmatization of mental illnesses. The Canadian Journal of Psychiatry. 2012;57(8):457-463.
13. Klarić M, Lovrić S. Methods to fight mental illness stigma. Psychiatria Danubina. 2017;29(suppl. 5):910-917.
The stigma surrounding mental and behavioral health challenges keeps many people from seeking the help they need. This stigma can be felt in painful instances of stereotyping, prejudice, and/or discrimination. One way to help de-stigmatize mental illness is by using person first language (PFL).
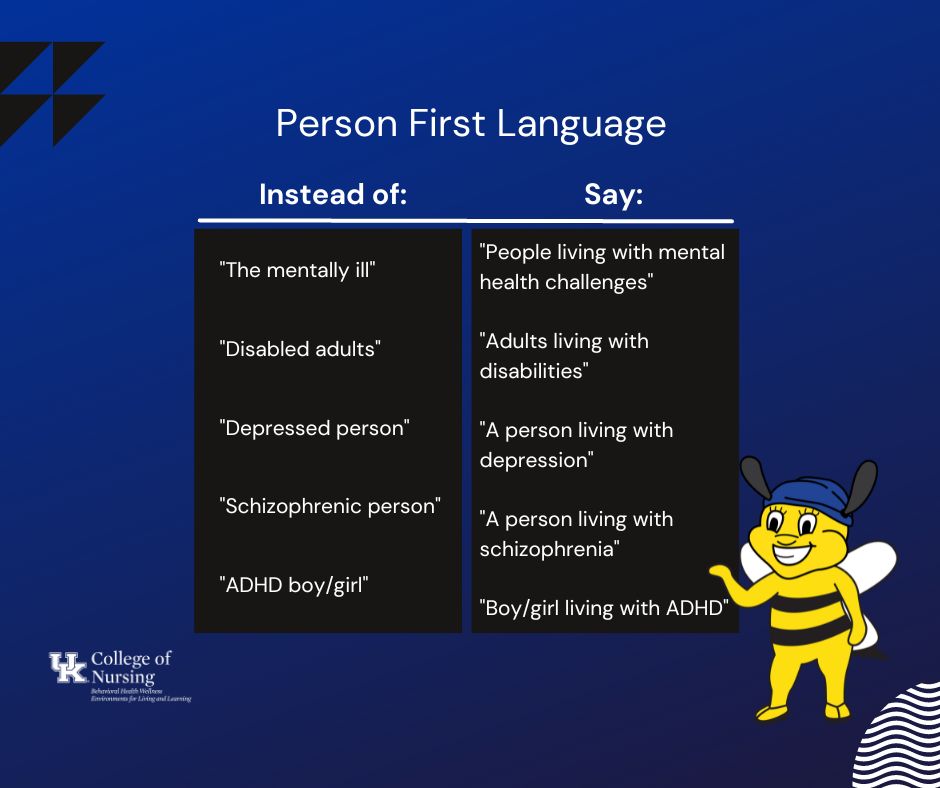
PFL is a mindful way of communicating that expresses knowledge and respect for people living with mental or behavioral health challenges or disabilities. PFL uses phrases such as “a person living with a mental health challenge,” or “individuals living with disabilities,” instead of phrases that identify people based solely on their challenge or disability, such as “the disabled” or “the mentally ill.” PFL encourages the use of words that prioritize the person first and their diagnosis second. This way of communicating differentiates that a person’s diagnosis does not define who they are.
Living with a mental or behavioral health challenge is only one part of a person’s identity. That’s why PFL is important. As Hecht et al. explain, caring and considerate language can “be harnessed to reduce mental health stigma” (2022). Phrases such as ‘afflicted with,’ ‘suffers from,’ and ‘victim of’ imply tragedy and do not consider other aspects of that person’s full story. While it can seem wordy to say "a person living with mental health challenges" rather than saying "a mentally-ill person," this subtle change is impactful and important.
Want to practice? We’re cheering you on! Use this graphic organizer to help integrate PFL into your everyday life.
Language can reinforce stigma OR emphasize individuality, equality, and respect. Consider using PFL in your conversations! You can be an agent of change just by staying mindful.
The Behavioral Health Wellness Environments for Living and Learning (BH WELL) research team exists to promote behavioral health and wellness among individuals facing behavioral health challenges.
References
Fox, A. B., Earnshaw, V. A., Taverna, E. C., & Vogt, D. (2018). Conceptualizing and Measuring Mental Illness Stigma: The Mental Illness Stigma Framework and Critical Review of Measures. Stigma and health, 3(4), 348–376.
Hecht, Marlene, Andrea Kloß, and Anne Bartsch. “Stopping the Stigma. How Empathy and Reflectiveness Can Help Reduce Mental Health Stigma.” Media psychology. 25.3 (2022): 367–386. Web.
Have you ever thought your child may be exhibiting signs of Attention Deficit Hyperactivity Disorder (ADHD) but you simply aren’t sure? This video blog is for you! It shares the signs of ADHD along with what unmanaged ADHD symptoms may look like. It also reviews different forms of ADHD and potential differences between boys and girls living with ADHD.
Read Transcript
WHAT IS ADHD?
Attention Deficit Hyperactivity Disorder (ADHD) is the most common neurobehavioral disorder diagnosis worldwide, affecting over 5% of children. Think of “neurobehavioral” as something happening in your brain that is impacting how you behave.
COMMON CHARACTERISTICS OF ADHD
ADHD is characterized by developmentally inappropriate levels of:
Hyperactivity/impulsivity and/or
Inattention
There are two main categories of symptoms for ADHD (inattention and/or hyperactivity/impulsivity).
Three kinds of presentations can occur: Combined (enough symptoms from both categories), predominantly inattentive, or predominantly hyperactive-impulsive.
A child exhibiting ADHD symptoms may experience negative impacts such as:
Academic and social difficulties (i.e., struggles in school),
Rejection by their peers, and
Challenges making friends.
In addition to these challenges, children at risk for ADHD are more likely to have poor social skills. Because of this challenge, they may be viewed as
Bossy,
Inflexible,
Controlling,
Easily frustrated,
Inattentive
Couple that with struggling to cooperate, share, or take turns, and a child’s social life can take a nosedive.
Children exhibiting all symptoms of ADHD may be seen as more likely to start fights and arguments. Not only do children at risk of living with ADHD struggle socially but they may also have underlying social cognitive difficulties, such as difficulty recognizing social cues like tones of voice and facial expressions.
It is also important to note that there is a form of ADHD that is predominately inattentive. A child living with predominately inattentive ADHD is more likely to be viewed as very shy.
WHAT ARE SOME DIFFERENCES IN ADHD SYMPTOMS BETWEEN BOYS AND GIRLS?
Due to differences in symptoms between sexes, ADHD and comorbidities are more likely to be noticed by parents and teachers in boys than in girls. For example, boys tend to exhibit higher levels of rule-breaking and externalizing behaviors when compared to girls. Also, parents of boys may expect ADHD behaviors to last for a shorter amount of time than parents of girls. As girls exhibit fewer externalizing symptoms compared to boys, girls’ ADHD symptoms and social difficulties may be less noticeable during an intervention.
A girl might be off task but just seems to be dazed or daydreaming rather than exhibiting hyperactive behaviors. Without noticing these symptoms, girls may miss parts of an intervention, potentially decreasing its overall effectiveness.
POTENTIAL TREATMENTS
Medication is commonly used to treat ADHD symptoms, but medication alone does not resolve social difficulties. Behavioral interventions may be necessary to improve social problems. An occupational therapist, or "OT," can help children living with ADHD improve a number of skills, including:
Controlling energy levels (whether experiencing hyperactivity or low points)
Increased organization
Improved physical coordination and
An improved ability to do everyday tasks - such as taking a shower, organizing their backpack, or making their bed - quickly and well.
Why the need for behavioral interventions?
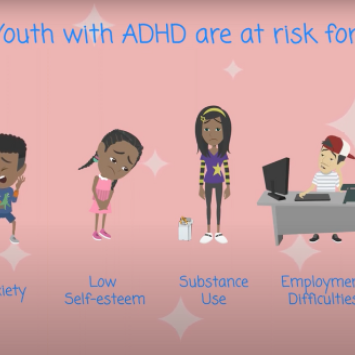
Up to 50% of children with ADHD are rejected by their peers, putting them at risk for long-term challenges with depression, anxiety, low self-esteem, substance use, employment difficulties, and school failure.
When ADHD symptoms are not addressed in childhood, they can prolong into adulthood and even intensify. However, mastering skills, such as emotional regulation, the ability to focus during social interactions, being aware of how others feel, and learning to read social cues, can allow children to better integrate with their peers. The passage of time, may not necessarily improve social challenges associated with ADHD. So, it is important to notice and treat these social difficulties as early as possible to prevent future negative consequences as a child develops.
WHAT CAN I DO AS A PARENT IF I THINK MY CHILD IS AT-RISK FOR ADHD?
Having a parent helping a child with social skills at home may aid in the internalizing of the intervention’s desired learning outcomes. However, in addition, it is important to find a behavioral health provider that interacts well with your child. A behavioral health provider will be able to assess your child’s risk for ADHD and other behavioral health challenges and will be able to provide the professional care your child needs!
References
Abikoff, H. B., Jensen, P. S., Arnold, L. L. E., Hoza, B., Hechtman, L., Pollack, S., Martin, D., Alvir, J., March, J. S., Hinshaw, S., Vitiello, B., Newcorn, J., Greiner, A., Cantwell, D. P., Conners, C. K., Elliot, G., Greenhill, L. L., Kraemer, H., Pelham, W. E., Jr., … Wigal, T. (2002). Observed classroom behavior of children with ADHD: Relationship to gender and comorbidity. Journal of Abnormal Child Psychology, 30, 349–359. https://doi-org.ezproxy.uky.edu/10.1023/A:1015713807297
Bellanti, C. (2009). Fostering social skills in children with ADHD. Brown University Child & Adolescent Behavior Letter, 25, 1–6. https://doi.org/10.1002/cbl.20083
Bussing, R., Schoenberg, N. E., Rogers, K. M., Zima, B. T., & Angus, S. (1998). Explanatory Models of ADHD: Do They Differ by Ethnicity, Child Gender, or Treatment Status? Journal of Emotional and Behavioral Disorders, 6, 233–242. https://doi.org/10.1177/106342669800600405
Carpenter Rich, E., Loo, S. K., Yang, M., Dang, J., & Smalley, S. L. (2009). Social functioning difficulties in ADHD: association with PDD risk. Clinical Child Psychology and Psychiatry, 14, 329–344. https://doi.org/10.1177/1359104508100890
DuPaul, G., & Weyandt, L. (2006). School‐based Intervention for Children with Attention Deficit Hyperactivity Disorder: Effects on academic, social, and behavioural functioning. International Journal of Disability, Development & Education, 53, 161–176. https://doi-org.ezproxy.uky.edu/10.1080/10349120600716141
Joelsson, P., Chudal, R., Gyllenberg, D., Kesti, A.-K., Hinkka-Yli-Salomäki, S., Virtanen, J.-P., Huttunen, J., Ristkari, T., Parkkola, K., Gissler, M., Sourander, A., & Hinkka-Yli-Salomäki, S. (2016). Demographic Characteristics and Psychiatric Comorbidity of Children and Adolescents Diagnosed with ADHD in Specialized Healthcare. Child Psychiatry & Human Development, 47, 574–582. https://doi-org.ezproxy.uky.edu/10.1007/s10578-015-0591-6
Mrug, S., Hoza, B., & Gerdes, A. C. (2001). Children with attention-deficit/hyperactivity disorder: Peer relationships and peer-oriented interventions. In D. W. Nangle & C. A. Erdley (Eds.), The role of friendship in psychological adjustment. (pp. 51–77). Jossey-Bass. https://doi.org/10.1002/cd.5
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: a systematic review and metaregression analysis. The American Journal of Psychiatry, 164, 942–948. https://doi.org/10.1176/ajp.2007.164.6.942
Rydell, A.-M. (2010). Family factors and children’s disruptive behaviour: an investigation of links between demographic characteristics, negative life events and symptoms of ODD and ADHD. Social Psychiatry & Psychiatric Epidemiology, 45, 233–244. https://doi-org.ezproxy.uky.edu/10.1007/s00127-009-0060-2
Wehmeier, P. M., Schacht, A., & Barkley, R. A. (2010). Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. Journal of Adolescent Health, 46, 209–217. https://doi-org.ezproxy.uky.edu/10.1016/j.jadohealth.2009.09.009
Willis, D., Siceloff, E. R., Morse, M., Neger, E., & Flory, K. (2019). Stand-alone social skills training for youth with ADHD: A systematic review. Clinical Child and Family Psychology Review, 22, 348–366. https://doi-org.ezproxy.uky.edu/10.1007/s10567-019-00291-3
Wilkes-Gillan, S., Bundy, A., Cordier, R., & Lincoln, M. (2016). Child outcomes of a pilot parent-delivered intervention for improving the social play skills of children with ADHD and their playmates. Developmental Neurorehabilitation, 19, 238–245. https://doi-org.ezproxy.uky.edu/10.3109/17518423.2014.948639
This is the first-hand story of a woman struggling with postpartum depression. She shares how it took her, "Five years. It took five years of convincing, cajoling, and near pleading for me to swallow a pill..."
Continue Reading Transcript
I grew up with a fear of mental illness and a deep suspicion of psychiatric drugs. Which is why it took a collective five years of persuasion by my caring therapists to swallow that little pill.
Flash forward to eight years later, when I’d gone cold turkey off those meds, popped out a baby, and was a manic mess. Things unraveled fast and there I was checking into the psychiatric hospital in the middle of the night, stumbling along behind a staff.
As we rounded the massive, high-ceilinged main room, a woman sat silently in a chair while another woman bustled softly nearby, and a few staff members chatted behind the desk. The bustling woman asked something like, “Do you want to go back to bed now, Lin?” The woman in the chair made a few small motions in response. Their conversation continued that way, the bustling woman speaking and the woman in the chair making tiny gestures in reply.
I shrank away from the woman in the chair. She must be a patient….like me. But I wasn’t like her, my manic brain insisted. I’d talk only to the staff. I then proceeded to initiate a loud, too-friendly conversation with the women behind the desk. THEY were who I could relate to, after all. Not this strange woman who sat silent and unblinking in the middle of the night.
Do you have a child with attention deficit hyperactivity disorder (ADHD)? Raising a child with ADHD can be anxiety-inducing, stressful, and exhausting. Children with ADHD may find it challenging to listen, focus, or stay calm. This may lead some parents to feel as if they are caught in a cycle of feeling frustrated, expressing the frustration in the presence of the child, and then feeling guilty for having outwardly expressed their frustration.
The following tips can help you and your child reduce some of the stress and anxiety that may accompany day-to-day challenges related to an ADHD diagnosis.
Take care of yourself.
In order to help a child with ADHD, take care of yourself first. Eat a balanced diet, get adequate sleep, exercise regularly, and find ways to reduce stress throughout the day.
Stay calm and focused.
Show your child how to stay calm and focused by modeling these behaviors. If your child is struggling, watching you manage your own emotions may calm them and help diffuse the situation. Staying calm will also help your child connect with you.
Keep a positive attitude.
Make a list of positive and unique things about your child. This will help you remain positive amidst challenges. Be sure to encourage your child in areas where they excel.
Believe in your child.
Believe that your child can learn and succeed on a daily basis and show this belief through your words and actions!
Follow a structured routine.
Set simple routine habits for your child's sleep, meals, play, and homework. Before going to bed, have your child prepare for the next day by picking out clothes, packing lunch, and having their backpack ready to go.
Use clocks/ timers to help your child manage their time.
Children living with ADHD often need more time to complete tasks as compared to children not living with ADHD. Combine that with difficulty focusing and it may seem like tasks never get done. However, clocks and timers are effective tools for helping a child with ADHD manage their time and transition smoothly from one activity to another. Place clocks or timers in your child’s bedroom and in other areas of the house. Using these reminders will help your child manage their time while doing homework, playing, eating meals, and getting ready for bed. It is important to allow your child enough time to finish a task; so, consider this when setting time limits or goals for your child.
Reduce distractions.
Provide a quiet place for your child to do homework.
Ask for help.
When you are feeling overwhelmed, ask for help from friends, family, or neighbors. You don’t have to do everything alone.
Ask for support from a healthcare professional.
Your child’s healthcare provider can help you understand ADHD and give you tools and strategies to help your child.
Taking care of yourself, managing your own emotions, creating a routine for your child, and asking or seeking for help are the best things you can do to help you help your child who is living with ADHD.
References
Corcoran, J., Schildt, B., Hochbrueckner, R., Abell, J. (2017). Parents of Children with Attention Deficit/Hyperactivity Disorder: A Meta-Synthesis, Part I. Child and Adolescent Social Work Journal, 34(4), 281-335.
Peasgood, T., Bhardwaj, A., Brazier, J. E., Biggs, K., Coghill, D., Daley, D., & Sonuga-Barke, E. J. (2020). What Is the Health and Well-Being Burden for Parents Living with a Child with ADHD in the United Kingdom? Journal of Attention Disorders, 1087054720925899.
Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). (n.d.). Parenting a Child with ADHD. Retrieved from https://chadd.org/for-parents/overview/
Lovoria Williams, Ph.D., FNP-BC, FAANP, is an Associate Professor in the UK College of Nursing. She is also a part of the BH WELL faculty team. Her research focuses on delivering interventions to reduce health disparities among minority and medically underserved populations. In this brief video, she shares her thoughts on finding a health provider that reflects your image and background.
Did you know 1 in 5 women experience completed or attempted rape during their lifetime? Want to learn more about sexual assault facts and the role of the sexual assault nurse examiner? Your journey begins here…
What is a SANE?
A registered nurse or advanced practice nurse that is certified to address the crime of sexual assault by implementing a process of high-quality medical care, accurate evidence collection, and support for sexual assault survivors.
Why are SANE’s important?
“Victims of violence and abuse require care from a health professional who is trained to treat the trauma associated with the wrong that has been done to them.” (IAFN)
What is sexual violence?
This type of violence comes in many forms including sexual harassment, stalking, sexual assault including sexual abuse of medical professionals, elder abuse, and sexual abuse of people with disabilities to name a few. SANE’s focus is on sexual assault or sexual abuse.
How big is the problem in the US?
Sexual assault happens in every community and affects people of all genders and ages. According to the National Sexual Violence Resource Center: Women aren’t the only victims. One in 71 men have experienced rape or attempted rape.
What age groups are affected?
1 in 3 women experienced attempted or completed rape for the first time between the ages of 11 and 17. For men, it is 1 in 4. Nearly 3 out of 4 adolescents who have been sexually assaulted know their attacker.
Myth or Fact?
There is a lot of information circulating about sexual violence and the people affected by it.
Here are some common myths:
Myth: Sexual assault is an act of lust and passion.
Fact: Sexual assault is about power and control.
Myth: If a victim doesn’t fight back, they must have wanted the assault.
Fact: Many survivors experience a “freeze response” during an assault and are unable to move or speak.
Myth: A lot of victims lie about being raped.
Fact: Two to 10% are false reports.
Myth: Sex workers cannot be raped because they are selling sex.
Fact: Sex workers have the right to give and withhold consent to any sexual activity.
Myth: People with disabilities are at low risk for sexual assault.
Fact: People with disabilities are victims of sexual assault twice as much as people without.
Myth: Wearing revealing clothing, behaving provocatively, or being under the influence means the victim was “asking for it”.
Fact: The perpetrator selects the victim, no one “asks” to be raped.
Why is sexual assault often not reported?
Some of the most common reasons include:
Fear of not being believed
Being afraid of retaliation
Shame or fear of being blamed
Pressure from others
Distrust toward law enforcement
Desire to protect the attacker
My role as a SANE is to provide care to victims of sexual assault and address the trauma that may have occurred with the assault. In addition, my role involves collecting evidence that can be used in a criminal trial if the victim wishes. I want survivors of sexual assault to know they have options and I will uphold their confidentiality and respect their choices. I want to support the survivor as much as I can at the beginning of their recovery process.