Emotional wellness is the awareness and ability to express feelings and emotions in healthy ways. It is the sense of fulfillment and achievement in life and includes self-acceptance, self-awareness, self-esteem, and optimism.
Quality of Life: One’s satisfaction with life in terms of self-concept, hopes for oneself, health, functional abilities, and socioeconomic factors (American Occupational Therapy Association, 2020).
Many people have little to no advance notice of when their life will end. However, others may be told, “We’ve done all we can do medically. What can we do to help make you more comfortable as you near end-of-life?” In those days, discussions occur (and rightfully so) about pain management, medical findings, treatments, associated costs, and more. But does anyone address mental wellness? Life satisfaction, and the hope that accompanies it, demands focused attention to mental wellness.
As a loved one nears the end-of-life, one’s ability to perform daily tasks often decreases, and the activities that are most meaningful change. For example, functional mobility may decrease or be lost completely. While this impacts daily life greatly, there are ways to modify meaningful tasks that encourage continued participation. For example, while your loved one may not be able to take an evening walk, they might enjoy chair aerobics or a drive to familiar parks or green spaces. Maintaining gentle activity may help decrease joint pain and increase your loved one’s ability to maintain personal hygiene. For most people who are nearing the end of life, independence often equals increased quality of life.
It is also common for a loved one to experience emotional difficulties, such as depression and anxiety, due to the stressors associated with end-of-life. These types of emotional difficulties can make completing self-care tasks, participating in social events, and participating in many other typical daily experiences difficult or seemingly impossible. However, understanding that emotional difficulties are common among individuals nearing end-of-life allows for preventative treatment that may lessen the occurrence of these difficulties. Preventative treatment includes seeking the support of a mental health professional who can help process thoughts and feelings. The practice of mindfulness in one’s daily routine can help to focus on simple daily accomplishments and build a sense of gratitude. Simply encouraging participation in life activities may help combat these emotional difficulties because they are engaging in one of their favorite activities with you, thereby increasing life satisfaction.
Importantly, as you support your loved one through end-of-life experiences, remember that you, too, are experiencing loss. Take time to get the support you need as a caregiver. Struggling with your own emotions? Consider professional counseling. Talk to a friend. Extra energy? Go for that walk. Racing thoughts? Take time to stop and breathe. Be mindful.
Does end-of-life mental wellness matter? Yes. In fact, mental wellness probably matters more at that time than at any other time.
If you or someone you love is experiencing end-of-life and would benefit from mental wellness support, call SAMHSA’s National Helpline at 1-800-662-HELP (4357).
References
American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010. https://doi.org/10.5014/ajot.2020.74S2001
Hammill, K., Bye, R., & Cook, C. (2019). Occupational engagement of people living with a life‐limiting illness: Occupational therapists’ perceptions. Australian Occupational Therapy Journal, 66(2), 145–153. https://doi.org/10.1111/1440-1630.12557
Smith, S., Wilson, C. M., Lipple, C., Avromov, M., Maltese, J., Siwa, E., Colombo, R., & Seidell, J. W. (2019). Managing palliative patients in inpatient rehabilitation through a short stay family training program. American Journal of Hospice and Palliative Medicine, 37(3), 172–178. https://doi.org/10.1177/1049909119867293
We have all likely experienced the shame, pain, and sting of being stigmatized at some point. Stigmatization appears in diverse forms-including derogatory comments about skin tone, hair texture, or body size; denial of resources due to social standing; and devaluation of persons because of sexual/gender identity, religious affiliation, or political preferences. Regardless of its form, stigmatization is never productive and poses a considerable threat to mental health and well-being.
There are an estimated 52.9 million adults (21.0% of the adult population) suffering from mental health disorders (MHDs) in the United States (1). Among those with mental health disorders,~ 17 million are also diagnosed with a cooccurring …
"All have their worth and each contributes to the worth of the others." The Silmarillion, by J.R.R. Tolkien In my view, this quote captures the drive to achieve equity in mental health care. All people have worth, and every person's worth adds to the worth of every other per- son. Our psychiatric-mental health nursing care is driven by this absolute belief that all people are of equal worth, of equal value.
Trauma exposure is prevalent in the general population, but healthcare workers may be at greater risks for additional work-related trauma. Trauma is a known risk factor for substance use, particularly tobacco and risky alcohol use. Few studies have examined the relationship between trauma and substance use in healthcare workers. Among healthcare workers, the aims of our study were to examine (a) frequency of current tobacco use and risky alcohol use, (b) frequency and types of traumatic experiences, and (c) the associations between trauma experiences and current tobacco and risky alcohol use controlling for demographic factors. This study is a secondary analysis of cross-sectional survey data from healthcare workers (N = 850) in an academic medical center.
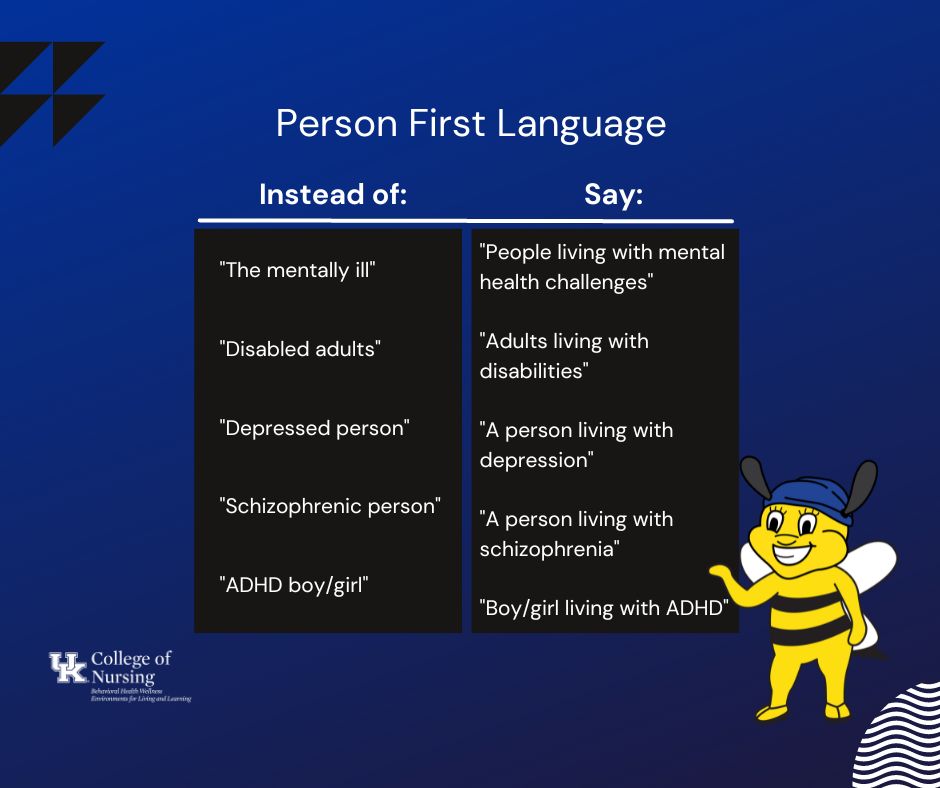
The stigma surrounding mental and behavioral health challenges keeps many people from seeking the help they need. This stigma can be felt in painful instances of stereotyping, prejudice, and/or discrimination. One way to help de-stigmatize mental illness is by using person first language (PFL).
PFL is a mindful way of communicating that expresses knowledge and respect for people living with mental or behavioral health challenges or disabilities. PFL uses phrases such as “a person living with a mental health challenge,” or “individuals living with disabilities,” instead of phrases that identify people based solely on their challenge or disability, such as “the disabled” or “the mentally ill.” PFL encourages the use of words that prioritize the person first and their diagnosis second. This way of communicating differentiates that a person’s diagnosis does not define who they are.
Living with a mental or behavioral health challenge is only one part of a person’s identity. That’s why PFL is important. As Hecht et al. explain, caring and considerate language can “be harnessed to reduce mental health stigma” (2022). Phrases such as ‘afflicted with,’ ‘suffers from,’ and ‘victim of’ imply tragedy and do not consider other aspects of that person’s full story. While it can seem wordy to say "a person living with mental health challenges" rather than saying "a mentally-ill person," this subtle change is impactful and important.
Want to practice? We’re cheering you on! Use this graphic organizer to help integrate PFL into your everyday life.
Language can reinforce stigma OR emphasize individuality, equality, and respect. Consider using PFL in your conversations! You can be an agent of change just by staying mindful.
The Behavioral Health Wellness Environments for Living and Learning (BH WELL) research team exists to promote behavioral health and wellness among individuals facing behavioral health challenges.
References
Fox, A. B., Earnshaw, V. A., Taverna, E. C., & Vogt, D. (2018). Conceptualizing and Measuring Mental Illness Stigma: The Mental Illness Stigma Framework and Critical Review of Measures. Stigma and health, 3(4), 348–376.
Hecht, Marlene, Andrea Kloß, and Anne Bartsch. “Stopping the Stigma. How Empathy and Reflectiveness Can Help Reduce Mental Health Stigma.” Media psychology. 25.3 (2022): 367–386. Web.
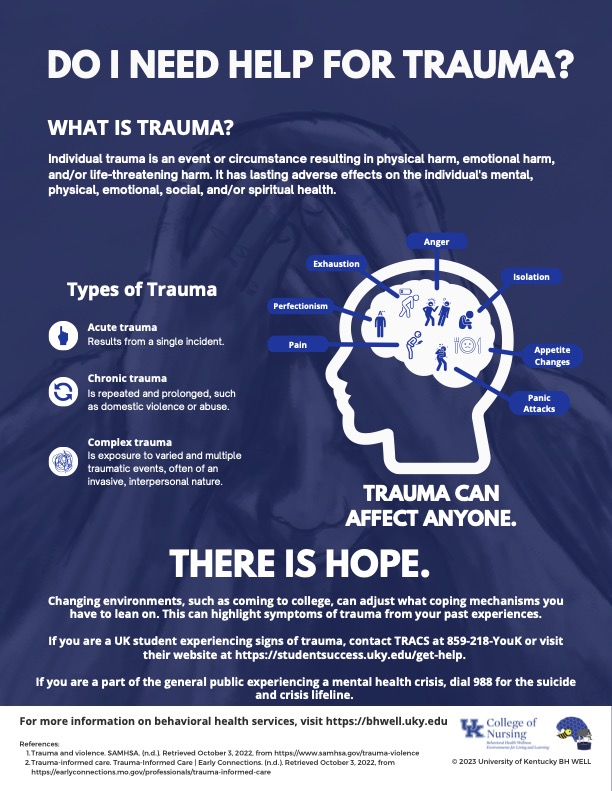
Individual trauma is an event or circumstance resulting in physical harm, emotional harm, and/or life-threatening harm. The event or circumstance has lasting adverse effects on the individual's mental, physical, emotional, social, and/or spiritual health. (1) Trauma can affect anyone regardless of age, gender, socioeconomic status, race, ethnicity, or sexual orientation.
There are three types of trauma: acute, chronic, and complex. Acute trauma results from a single incident. Chronic trauma is repeated and prolonged, such as domestic violence or abuse. Complex trauma is exposure to varied and multiple traumatic events, often of an invasive, interpersonal nature. (1) Any type of trauma may make it more difficult to participate in the responsibilities of everyday life.
Warning signs of trauma can include:
Excessive anger or irritability
Unusual startle reactions
Significantly increased or reduced appetite
Exhaustion
Aggression (physical or verbal)
Regular tardiness/absence from class or work
Perfectionist or controlling behavior
Difficulty concentrating
Frequent headaches or stomach aches
Low self-confidence
Hoarding (snacks, school supplies)
Risky behavior (substance use, sex)
Panic attacks
Alienation from peers (self-isolation or inability to relate/make friends)
If you or someone you love may be experiencing signs of trauma, there is hope. Contact the Center for Support and Intervention at (859) 257-3755.
BH WELL exists to promote behavioral health and wellness among individuals facing behavioral health challenges. Learn more about BH WELL at https://bhwell.uky.edu. Follow us on social media.
I’m a jack-in-the-box, safe and secure in the confines of my box. Sadly, this safety and security are short-lived. Outside the box, the crank is constantly turning, turning, and without warning, I’m thrust into an intense rollercoaster of fear, guilt, and anger.
Read Transcript
I’m a jack-in-the-box, safe and secure in the confines of my box. Sadly, this safety and security are short-lived. Outside the box, the crank is constantly turning, turning, and without warning, I’m thrust into an intense rollercoaster of fear, guilt, and anger. I’m triggered by a sight, a smell, a taste, or a noise I’m thrust into my past trauma, reliving each physical sensation and emotional experience either through flashbacks while awake or through nightmares while asleep. I’m engulfed by my flashbacks and nightmares, struggling to snap out.
As I realize there is no immediate threat, I begin to calm down. My body loses all energy and collapses, mentally exhausted. At the first opportunity, I flee back into my box, willing myself to brave the moments ahead. Despite feeling composed back in the box, I’m left feeling on edge and on guard. When will I be propelled out of my box again? What will the trigger be that time? Where will I be and who will be around me? Not knowing when I will burst out of the box not only alarms me, but also alarms those who exist outside of the box: my loved ones, my coworkers, or even strangers on the street or in the store.
The triggers, flashbacks, and nightmares happen again and again over months and months. Over time, I try to take myself away from anything and everything that reminds me of distressing memories. Sometimes I am numb to my feelings. No matter what I do to avoid my triggers, I’m reminded of my experiences again and again.
That’s why I decided to get help! My mental healthcare provider helped me through a plan that involved some medications and therapy to help with my problem. I learned to recognize my triggers and gained some skills to take care of the challenges with my feelings, thoughts and behaviors. Then one day, I popped out of my box and realized ‘it is just a box’. I realized my bad memories can exist alongside new and happier memories that I am making now. Then I decided that while the box remains, and while the bad memories are still there, I can choose to face my trauma while being supported by my mental healthcare provider. The more I learn about facing my trauma, the more I’m reminded that I don’t have to pop out of anything. I can just be.
If you or someone you know is experiencing post-traumatic stress disorder (PTSD), there is hope. Contact your health provider or call the National Helpline at 1-800-662-HELP (4357) supported by the Substance Abuse and Mental Health Services Administration (SAMHSA).
References
Administration for Community Living. (n.d.). MHDD: Post-Traumatic Stress Disorder. The Mental Health and Developmental Disabilities National Training Center. Retrieved June 7, 2022, from https://rise.articulate.com/share/_krWkjSaEunOmpN8wSRR6k2Zl9WK Hwzz#/
Cleveland Clinic. (2021, June 15). Living With PTSD? How to Manage Anxiety and Flashbacks. Cleveland Clinic. Retrieved June 7, 2022, from https://health.clevelandclinic.org/living-with-ptsd-how-to-manage-anxiety-and-flashbacks/
Torres, F. (2020, August). What is Posttraumatic Stress Disorder (PTSD)? American Psychiatric Association. Retrieved June 7, 2022, from https://psychiatry.org/patients-families/ptsd/what-is-ptsd
U.S. Department of Health and Human Services. (2019, May). Post-Traumatic Stress Disorder. National Institute of Mental Health. Retrieved June 7, 2022, from https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd
Why Youth Mental Health is Essential to Healthy Development
National Youth Mental Health Awareness Month serves as a reminder each February that caring for a young person’s mental health is of the utmost importance. Youth mental health is essential to healthy development.
However, millions of youth, defined as ages 12 to 17, living with mental or behavioral health challenges go undiagnosed and lack support. Youth mental health disorders come in all shapes and sizes such as anxiety, depression, post-traumatic stress disorder (PTSD), and eating disorders. Substance use disorders, such as the use of alcohol, tobacco, and marijuana, are also prevalent.
Youth Mental Health Stats That May Shock You
In 2021, 35% of youth experienced a major depressive episode (MDE) in the last year and 27%of the youth who experienced an MDE used alcohol, tobacco, marijuana or other drugs. This would be like one-third of youth experiencing a broken leg, and a quarter of those youth also using a substance. The youth should receive medical care (i.e. x-rays, casts or boots) and be referred to a counselor regarding the drug use. However, with MDEs, one-third of our youth are not receiving mental health care.
Less than half (44%) of the youth who experienced an MDE with severe impairment received treatment for depression in the past year. Impairment is measured across 4 areas of life: chores at home, school or work, close relationships with family and social life. Of the youth population reported as having experienced an MDE in the last year and alcohol, tobacco, marijuana, or other drug use, 4 in 10 youth did not receive services (1).
We would not leave the youth alone to heal their own broken legs. Similarly, we cannot assume that youth living with depression or depression and substance use can manage their own mental and behavioral health care.
Awareness about the importance of youth mental health throughout the developmental years is important. Here are a few free resources that can empower youth to live their best lives!
Have fun while you learn more about how you can be well with coloring books.
While resources such as fun educational videos and comic or coloring books can be helpful, it is important to seek mental health care when needed. Youth, who seek mental health services, do so most often for feelings of depression, thinking of or attempting suicide, or because of problems at home or with family. There are many youth experiencing a mental or behavioral health challenge without mental health services or support. If you or a youth you know is experiencing a mental or behavioral health challenge, there is hope! Call 1-800-662-HELP (4357) or dial 988. You can also call the National Mental Health Hotline at 1-866-903-3787. For suicide prevention, call 800-273-TALK (8255) or call the 24-hour National Suicide Crisis Hotline at 800-SUICIDE.
The Behavioral Health Wellness Environments for Living and Learning (BH WELL) research team exists to promote behavioral health and wellness among individuals facing behavioral health challenges. Click here for more information about BH WELL. Follow us on social media.
One day, about five years ago, while resting and eating the previous night’s leftovers with my college roommate and lifelong friend Abby, we came across a video on how to take old candle jars and turn them into pots for plants. We boiled the leftover wax, removed it from the old candle jars, and set them aside. Then, we visited a local home improvement store.
Having a limited budget, we both picked two discount cacti on the verge of death, about 50 cents each, shared a bag of potting soil, and went home to continue our repurposing project. After potting the struggling cacti into the old candle jars, they thrived! The cacti grew with us over the years as we moved from house to house and grew into young professionals.
Today, my home has roughly two hundred plants of a wide variety of species, colors, shapes and sizes. My old cacti from the candle jar is affectionately named “Richard”. He has remained in my home for the past five years, living in ten different pots over the years. He never stops growing! Moreover, my tallest indoor plant, a Bird of Paradise (Strelitzia Reginae), is about seven feet tall. My smallest plant, a lithop (part of the Aizoaceae family native to Southern Africa), is the size of a quarter. For me, plants represent responsibility, fragility, dependency and hope. Plants demand their caregivers be responsible for them. Yes, a plant receives some of what it needs organically, like absorbing sunlight; but ultimately, if a plant is going to stay in an unnatural environment, we must adjust the environment to meet its needs. Plants can be fragile and easily harmed. Too much light, not enough humidity, overwatering, or pulling roughly at a stem are all ways plants can be harmed. I may have given you pause in considering gardening and raising indoor plants given the required responsibilities; but, you have yet to hear the best part. The best thing that plants do is to provide undeniable hope.
Do you recall the devastating nuclear disaster in Chernobyl? Against all odds, guess what was recently discovered in the area? Native plants. Martin Hajduch, a plant biologist for the Slovak Academy of Sciences, conducted a study on soybeans growing near Chernobyl. The soybeans were so resilient, they adapted to the soil conditions and grew despite all odds. Isn’t that incredible? Imagine if we had the strength of a tiny, seemingly insignificant, soybean. Plants are hope!
Other studies have shown the mental and physical health benefits of plants. In a review by Hall and Knuth (2019), emotional and mental health benefits of plants included decreased depression, reduced anxiety and stress, enhanced memory, and improved creativity and self-esteem, to name a few. Native American tribes use sweet grass to promote emotional strength and dispel negative energy. Sensory gardens, sometimes known as healing gardens, are beneficial to individuals living with or without special educational needs. These gardens offer a variety of plants which appeal to all of the senses and promote positive reactions to new sights, sounds, smells and touch.
It’s an odd thing to say I have a kinship with plants, but I DO! They are magical. Want some magic in your life? Grab any kind of seed from your local home improvement store and plant it with a little dirt in a tiny paper cup or empty egg carton. Give the seed a little light, a little water and a lot of patience. The day it sprouts, you will experience the magic! As your plant grows, share cuttings with your friends. You will be amazed at the magic plants create in your life.
There is a quote that comes to mind when I catch my priorities shifting and I am no longer caring for myself, my plants and the Earth. It comes from a fellow member of the Kentucky Wild Ones Chapter, a chapter of the national organization that studies and fights to preserve native plants for the health of our state.
“No matter what you encounter in the years to come, do not forget to look above at the sky and marvel at the clouds and the stars… Look about and note the individuality of every tree - the architecture of its branches, texture of its bark, venation of its leaves. All these things may be oblivious of us, but we do not need to be oblivious of them. This is what we belong to, and what grounds our sense of self.”
Anne Lubber
That, I believe, is magic! Plants remind us to pause and appreciate the details around us. So, what are you still doing here? Go plant a seed. Then, go share the magic of plants with the world!
References
Charles Hall, Melinda Knuth; An Update of the Literature Supporting the Well-Being Benefits of Plants: A Review of the Emotional and Mental Health Benefits of Plants. Journal of Environmental Horticulture 1 March 2019; 37 (1): 30–38.
Elsevier. (2012, April 19). The influence of sensory gardens on the behaviour of children with special educational needs. Procedia - Social and Behavioral Sciences. Retrieved January 18, 2023, from https://reader.elsevier.com/reader/sd/pii/S187704281200835X?token=C22C57413BFBC5B6367119D246E1E6740D2E7C055871565963437AC8B4D5D05C68A8864E55807FF12D46E462346C4B9B&originRegion=us-east-1&originCreation=20221201165408
How Plants Survived Chernobyl. Science. (n.d.). Retrieved January 18, 2023, from https://www.science.org/content/article/how-plants-survived-chernobyl
Sweet Grass has a pretty sweet history of health and Wellness. Beekman 1802. (n.d.). Retrieved January 18, 2023, from https://beekman1802.com/blogs/almanac/sweet-grass-has-a-pretty-sweet-history-of-health-and-wellness