Physical well-being is how one takes care of their body through proper nutrition, exercise, sleep, hydration, medical checkups, safe sex, and weight management.
Did you know 1 in 5 women experience completed or attempted rape during their lifetime? Want to learn more about sexual assault facts and the role of the sexual assault nurse examiner? Your journey begins here…
What is a SANE?
A registered nurse or advanced practice nurse that is certified to address the crime of sexual assault by implementing a process of high-quality medical care, accurate evidence collection, and support for sexual assault survivors.
Why are SANE’s important?
“Victims of violence and abuse require care from a health professional who is trained to treat the trauma associated with the wrong that has been done to them.” (IAFN)
What is sexual violence?
This type of violence comes in many forms including sexual harassment, stalking, sexual assault including sexual abuse of medical professionals, elder abuse, and sexual abuse of people with disabilities to name a few. SANE’s focus is on sexual assault or sexual abuse.
How big is the problem in the US?
Sexual assault happens in every community and affects people of all genders and ages. According to the National Sexual Violence Resource Center: Women aren’t the only victims. One in 71 men have experienced rape or attempted rape.
What age groups are affected?
1 in 3 women experienced attempted or completed rape for the first time between the ages of 11 and 17. For men, it is 1 in 4. Nearly 3 out of 4 adolescents who have been sexually assaulted know their attacker.
Myth or Fact?
There is a lot of information circulating about sexual violence and the people affected by it.
Here are some common myths:
Myth: Sexual assault is an act of lust and passion.
Fact: Sexual assault is about power and control.
Myth: If a victim doesn’t fight back, they must have wanted the assault.
Fact: Many survivors experience a “freeze response” during an assault and are unable to move or speak.
Myth: A lot of victims lie about being raped.
Fact: Two to 10% are false reports.
Myth: Sex workers cannot be raped because they are selling sex.
Fact: Sex workers have the right to give and withhold consent to any sexual activity.
Myth: People with disabilities are at low risk for sexual assault.
Fact: People with disabilities are victims of sexual assault twice as much as people without.
Myth: Wearing revealing clothing, behaving provocatively, or being under the influence means the victim was “asking for it”.
Fact: The perpetrator selects the victim, no one “asks” to be raped.
Why is sexual assault often not reported?
Some of the most common reasons include:
Fear of not being believed
Being afraid of retaliation
Shame or fear of being blamed
Pressure from others
Distrust toward law enforcement
Desire to protect the attacker
My role as a SANE is to provide care to victims of sexual assault and address the trauma that may have occurred with the assault. In addition, my role involves collecting evidence that can be used in a criminal trial if the victim wishes. I want survivors of sexual assault to know they have options and I will uphold their confidentiality and respect their choices. I want to support the survivor as much as I can at the beginning of their recovery process.
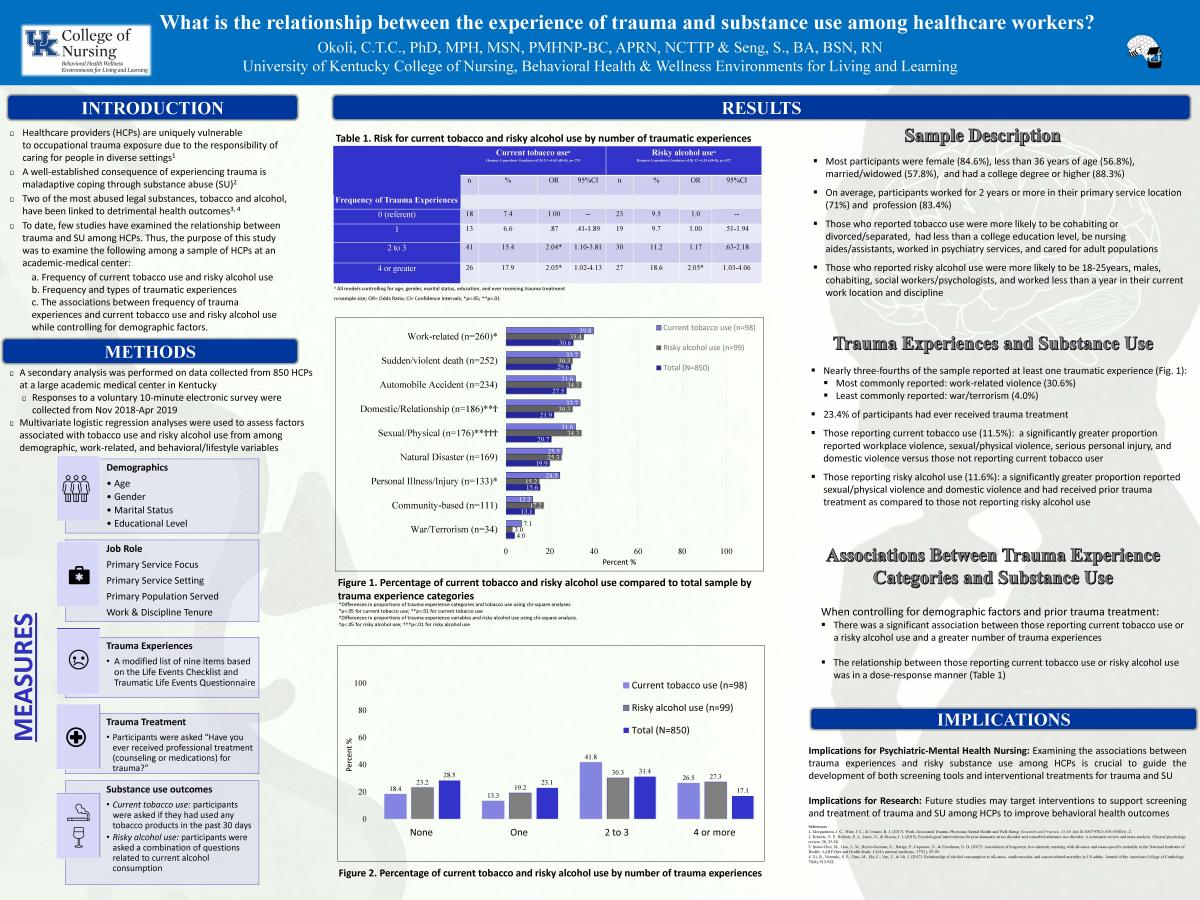
Healthcare providers (HCPs) are uniquely vulnerable to occupational trauma exposure due to the responsibility of caring for people in diverse settings.
People with psychiatric disorders (PDs) are disproportionately affected by tobacco use and its associated harms. Although several unique risk factors are known for this population, few studies have examined differences based on urban or rural residence.
Objectives: We aim to examine factors associated with tobacco use and consumption among rural and urban patients with PDs.
Methods: This is a retrospective correlational study using clinical data of 2,060 patients admitted to a government inpatient psychiatric facility between January 1, 2016 and December 31, 2016. Information was obtained on demographics, rurality status, smoke free policy status, substance use history, psychiatric diagnosis, and history of tobacco use. Logistic and multilinear regression analyses were performed to examine factors associated with tobacco use and consumption, stratified by urban and rural status.
Results: Tobacco users were significantly more likely to reside in rural as compared to urban settings (67.2% vs. 58.8%; p<0.001). Factors significantly associated with tobacco use among the urban population were male sex, history of substance use and treatment, and externalizing disorder. Among the rural population, history of substance use and treatment, less than high school education, decreasing age, and shorter length of hospital stay increased the risk of tobacco use. White, less than high school education, and psychotic disorder were significantly correlated with greater tobacco consumption in the urban population. For the rural population, male and less than high school education were positively associated with increased tobacco consumption.
Conclusions: Although rural patients with PDs are more likely to use tobacco, they face similar risk factors as compared to their urban counterparts. This suggests the need to increase access to treatment for rural individuals with PDs to reduce such disproportionate tobacco use prevalence and related disease risk.
People with psychiatric disorders (PDs) have high risks for tobacco use and associated health effects; however, little is known about differences in tobacco use status and consumption by urban or rural residence. Among patients with PDs, we examined the association of smoke-free policy on tobacco use by rural/urban residence METHOD: A cross-sectional retrospective study (N = 2060) among patients in a psychiatric facility was conducted. Multi-logistic and multilinear regression analyses assessed differences in outcomes stratified by rural/urban status.
Results: Among rural residents, a substance use history (odds ratios [ORs[ = 2.82, 95% CI: 2.01-3.96), high school education (OR = 0.71, 95% CI: 0.51-0.98), older age (OR = 0.99, 95% CI: 0.98-1.00), and longer length of hospital stay (OR = 0.99, 95% CI: 0.98-1.00) were associated with tobacco use. Among urban residents, male sex (OR = 1.38, 95% CI: 1.02-1.86), a substance use history (OR = 2.61, 95% CI: 1.86-3.66), and externalizing disorder diagnosis (OR = 2.72, 95% CI: 1.35-5.48) correlated with tobacco use. Increased tobacco consumption among rural residents was associated with being male (β = 0.12, p = 0.007) and having less than a high school education (β = 0.14, P = 0.001). Whereas, White ethnicity (β = 0.14, p = 0.006), having less than a high school education (β = 0.11, p = 0.022), and a psychotic disorder diagnosis (β = 0.25, p = 0.038) were associated with greater tobacco consumption in urban residents. Smoke-free policy was not associated with tobacco use (OR = 1.08, 95% CI: 0.87-1.34) and consumption (β = 0.05, p = 0.134).
Conclusions: Despite higher rates of tobacco use among rural patients with PDs, they have similar risk factors as their urban counterparts. However, residing in a location with a smoke-free policy may not contribute to tobacco use behaviors among those with PDs.
We all want to stay healthy, happy, and resilient. So, how can we do this? Health and happiness require checking in with yourself to assess your needs. Think: “Am I eating well? Exercising? Stressed? Needing to say ‘no’ to some things?”. Stay tuned for a prescription to REST.
We all want to stay healthy, happy, and resilient. So, how can we do this? Health and happiness require checking in with yourself to assess your needs. Think: “Am I eating well? Exercising? Stressed? Needing to say ‘no’ to some things?”. Stay tuned for a prescription to REST.
Why do we fail to take care of ourselves? Haven’t we learned our limits by now? Our lives are impossibly busy. We balance jobs, family, and never-ending daily agendas. But self-care shouldn’t feel like a burdening To-Do list item. It’s a GIFT to yourself and helps you love those around you better. And it doesn’t take a lot of time!
Here are 12 tips to beginning your journey of practicing self-care:
Sleep well.
Your nightly routine can train your body to know it is time for bed. Being aware of what you consume close to bedtime is important. Sugar, caffeine, and distractions like television tend to keep you awake. Checking your email may also awaken stress and a work-mode mindset that can make it hard to fall asleep.
Heal your gut.
While this includes eating healthy, it is even more. This is being aware of your body’s reaction to certain foods. Stomach aches, digestive troubles, fatigue, brain fog, skin issues, headaches, emotional issues, weight changes, and food intolerance are all examples of gut health issues. There are many important elements to this process but knowing your food triggers is a great place to start.
Exercise daily.
We don’t want to sound like a broken record, but exercise has physical and mental benefits. It boosts mood, reduces stress and anxiety, and helps you gain muscle and strength. Exercise doesn’t have to take place at the gym. You can go for a walk while listening to a podcast, dance to your favorite playlist, play tennis with a friend, or practice yoga.
Eat a clean nourishing diet.
The food we eat controls our weight, can cause or prevent disease, and can keep our minds active. The right foods can even prevent memory loss and inflammation which have long term effects on the body. Some of the best foods to eat are fatty fish, blueberries, walnuts, pistachio nuts, green leafy vegetables, and broccoli. Hydration is equally important for your body and brain!
Learn to say “NO”.
In order for you to function at your peak in your job, with your family, or just in your own mental space, you have to be calm and rested. You cannot be your best self if you continue to say “yes” when your plate is too full. You will be irritably working out of stress or obligation and likely find yourself burnt out. Learn how to say “no” politely but firmly and with conviction, and keep practicing until it comes more naturally.
Take a trip.
Even if you’re not feeling particularly stressed, getting away can provide space to disconnect, relax, and reset. This doesn’t have to be far or costly. You can visit a friend, explore a nearby town, or go camping. The goal is to get out of your normal routine and do something that sounds fun to you.
Go outside.
Being outdoors can reduce stress, lower blood pressure, reduce fatigue, and overcome symptoms of depression and burnout. It also helps you sleep better, especially if you do something active such as hiking, walking, or gardening. Nature is one of the best resources for healing. Listen to the birds, notice the trees, feel the wind, and appreciate the changes in the weather.
Spend time with a pet.
From companionship to unconditional love, pets bring huge benefit to our lives. Dogs, cats, and horses especially can reduce anxiety, stress, and lower blood pressure. Often, pets are empathetic to our moods and can tell when we are not feeling well. They are called our ‘best friend’ for a reason!
Prioritize getting organized.
Declutter the things in your mind by writing them in a planner or calendar. Keep a running grocery list or to-do list so you never again have to stress about what you may be forgetting. (Just don’t forget the list!). Another quick organizational habit is to prepare keys, purses, backpacks, briefcases, and coats to be ready to go for the next morning. This gives your mind more room to be creative!
Prepare your own meals.
Make this an event. Cook. Fast food and pre-made meals lack sufficient nutrients and are often more calorie-dense than fresh meals made at home. Even if it’s once a week, try cooking a healthy meal. The recent rise in meal kits and meal delivery services may help you get started.
Read a book on self-care.
Instead of scrolling a news feed for entertainment, try reading a self-help or self-care book. This can help you slow down, improve your mood, and help you be mindful and present where you are. Listen to a podcast on resilience, self-care, and the science of self-care practices.
Schedule daily self-care time like an important appointment.
You wouldn’t cancel breakfast with your favorite author, would you? Then why are we so quick to sweep our self-care aside? Self-care can help you stay grounded and keep goals at the forefront of your mind. Start small. Wake up 15 minutes early to have a cup of delicious herbal or green tea and practice deep breathing. Or take a walk around the block on your lunch break. The more you practice incorporating self-care into your schedule, the better you can grow and prioritize the things most important to you. Aim to take 5 minutes 5 times a day to practice self-care. 5 X 5. It’s like rebooting your brain for better health and performance.
People with mental illness (MI) have a disproportionate tobacco-related disease burden and mortality. Tobacco-use rates in people with MI are nearly twice that of the general population. Reasons for tobacco-use in this population may be a result of diminished tobacco-related disease risk perceptions. The purpose of this study was to examine the reasons for tobacco-use and perceived tobacco-related health risks among psychiatric inpatients. A correlational design was employed to survey a convenient sample of 137 patients from a psychiatric facility in central Kentucky. Information obtained from participants included demographics, psychiatric diagnoses, tobacco-use and exposure history, medical illness history, reasons for tobacco-use, and tobacco-related illness risk perceptions. The primary reasons participants endorsed for tobacco-use were for stress reduction, followed by addiction, then boredom, psychiatric symptom control, social, and negative mood. In addition, about 72% of participants used tobacco to cope with MI symptoms and 52% to manage the side effects of their medications. Participants were most likely to endorse that tobacco-use caused lung disease (83.2%), heart disease (79.6%), cancer (77.4%), and premature mortality (79.6%) but were less likely to admit that it may cause addiction to other drugs (39.4%) or MI (23.4%). Given the high endorsement of tobacco-use for stress reduction and psychiatric symptom control, it is important for mental health nurses to properly educate consumers on tobacco addiction and evidence of its effects on mental health. Strategies to incorporate our study findings into routine mental health services may address the tobacco-use disparities experienced by people with MI.
Background and Objectives: Approximately 65% of psychiatric inpatients experience moderate-to-severe nicotine withdrawal (NW), a set of symptoms appearing within 24 hr after an abrupt cessation or reduction of use of tobacco-containing products in those using nicotine daily for at least a couple of weeks. The Minnesota Tobacco Withdrawal Scale (MTWS) is a widely used instrument for detecting NW. However, the psychometric properties of the MTWS have not previously been examined among patients with serious mental illness (SMI) undergoing tobacco-free hospitalization. The objective of this study was to examine the validity and reliability of the MTWS among patients with SMI during tobacco-free psychiatric hospitalization.
Methods: Reliability was tested by examining Cronbach’s α and item analysis. Validity was examined through hypothesis testing and exploratory factor analysis (N = 255).
Results: The reliability analysis yielded a Cronbach’s α coefficient of .763, an inter-item correlations coefficient of .393, and item-total correlations between .291 and .691. Hypothesis testing confirmed the construct validity of the MTWS, and an exploratory factor analysis yielded a unidimensional scale.
Conclusion: The MTWS demonstrated adequate reliable and valid psychometric properties for measuring NW among patients with SMI. Nurses and other healthcare professionals may use this instrument in clinical practice to identify patients with SMI experiencing NW. The MTWS is psychometrically sound for capturing NW during tobacco-free psychiatric hospitalization. Future research should examine the efficacy of the MTWS in measuring NW in this population over an extended period of hospitalization.
Purpose: Continued cigarette smoking after a major cardiac event predicts worse health outcomes and leads to reduced participation in cardiac rehabilitation (CR). Understanding which characteristics of current smokers are associated with CR attendance and smoking cessation will help improve care for these high-risk patients. We examined whether smoking among social connections was associated with CR participation and continued smoking in cardiac patients.
Methods: Participants included 149 patients hospitalized with an acute cardiac event who self-reported smoking prior to the hospitalization and were eligible for outpatient CR. Participants completed a survey on their smoking habits prior to hospitalization and 3 mo later. Participants were dichotomized into two groups by the proportion of friends or family currently smoking ("None-Few" vs "Some-Most"). Sociodemographic, health, secondhand smoke exposure, and smoking measures were compared using t tests and χ2 tests (P < .05). ORs were calculated to compare self-reported rates of CR attendance and smoking cessation at 3-mo follow-up.
Results: Compared with the "None-Few" group, participants in the "Some-Most" group experienced more secondhand smoke exposure (P < .01) and were less likely to attend CR at follow-up (OR = 0.40; 95% CI, 0.17-0.93). Participants in the "Some-Most" group tended to be less likely to quit smoking, but this difference was not statistically significant.
Conclusion: Social environments with more smokers predicted worse outpatient CR attendance. Clinicians should consider smoking within the social network of the patient as an important potential barrier to pro-health behavior change.
Bolívar, Hypatia A. PhD; Elliott, Rebecca J. BS; Middleton, William BS; Yoon, Jin H. PhD; Okoli, Chizimuzo T. C. PhD; Haliwa, Ilana MPH; Miller, Charles C. III PhD; Ades, Philip A. MD; Gaalema, Diann E. PhD
National lung cancer screening with low dose computed tomography (LDCT) uptake is suboptimal. One factor contributing to slow uptake is lack of awareness. Trained Community Health Workers (CHWs) may be effective in increasing lung cancer screening awareness among disparate populations, however little is known about the processes necessary to scale an intervention for implementation by CHWs in a new area. We examined implementation processes with the RE-AIM framework and pilot tested a CHW-delivered lung cancer education intervention based on the Health Belief Model. We measured pre-post participant knowledge, attitudes and beliefs regarding cancer screening, lung cancer stigma, and intent to obtain LDCT screening. We used community-engaged strategies to collaborate with a local health system, to identify CHWs. CHWs were trained to recruit participants and deliver the one-session lung cancer education intervention. Seven CHWs and eight community sites participated. Participants (n = 77) were female (53%) primarily low income (62.9%); tobacco use was high (36.9%). Post intervention changes in lung cancer screening knowledge (p = < .0001), attitudes regarding lung cancer screening benefit (p = .034) and lung cancer stigma. (p = .024) We learned important lessons that will be useful in subsequent scaling. Collaborating with a local health system is a promising method to disseminate a lung cancer screening education intervention.