Intellectual well-being is the ability to constantly expand upon one’s own knowledge through creative and stimulating activities and experiences and to share what is already known with others. It is the exercising of the mind.
We all want to stay healthy, happy, and resilient. So, how can we do this? Health and happiness require checking in with yourself to assess your needs. Think: “Am I eating well? Exercising? Stressed? Needing to say ‘no’ to some things?”. Stay tuned for a prescription to REST.
We all want to stay healthy, happy, and resilient. So, how can we do this? Health and happiness require checking in with yourself to assess your needs. Think: “Am I eating well? Exercising? Stressed? Needing to say ‘no’ to some things?”. Stay tuned for a prescription to REST.
Why do we fail to take care of ourselves? Haven’t we learned our limits by now? Our lives are impossibly busy. We balance jobs, family, and never-ending daily agendas. But self-care shouldn’t feel like a burdening To-Do list item. It’s a GIFT to yourself and helps you love those around you better. And it doesn’t take a lot of time!
Here are 12 tips to beginning your journey of practicing self-care:
Sleep well.
Your nightly routine can train your body to know it is time for bed. Being aware of what you consume close to bedtime is important. Sugar, caffeine, and distractions like television tend to keep you awake. Checking your email may also awaken stress and a work-mode mindset that can make it hard to fall asleep.
Heal your gut.
While this includes eating healthy, it is even more. This is being aware of your body’s reaction to certain foods. Stomach aches, digestive troubles, fatigue, brain fog, skin issues, headaches, emotional issues, weight changes, and food intolerance are all examples of gut health issues. There are many important elements to this process but knowing your food triggers is a great place to start.
Exercise daily.
We don’t want to sound like a broken record, but exercise has physical and mental benefits. It boosts mood, reduces stress and anxiety, and helps you gain muscle and strength. Exercise doesn’t have to take place at the gym. You can go for a walk while listening to a podcast, dance to your favorite playlist, play tennis with a friend, or practice yoga.
Eat a clean nourishing diet.
The food we eat controls our weight, can cause or prevent disease, and can keep our minds active. The right foods can even prevent memory loss and inflammation which have long term effects on the body. Some of the best foods to eat are fatty fish, blueberries, walnuts, pistachio nuts, green leafy vegetables, and broccoli. Hydration is equally important for your body and brain!
Learn to say “NO”.
In order for you to function at your peak in your job, with your family, or just in your own mental space, you have to be calm and rested. You cannot be your best self if you continue to say “yes” when your plate is too full. You will be irritably working out of stress or obligation and likely find yourself burnt out. Learn how to say “no” politely but firmly and with conviction, and keep practicing until it comes more naturally.
Take a trip.
Even if you’re not feeling particularly stressed, getting away can provide space to disconnect, relax, and reset. This doesn’t have to be far or costly. You can visit a friend, explore a nearby town, or go camping. The goal is to get out of your normal routine and do something that sounds fun to you.
Go outside.
Being outdoors can reduce stress, lower blood pressure, reduce fatigue, and overcome symptoms of depression and burnout. It also helps you sleep better, especially if you do something active such as hiking, walking, or gardening. Nature is one of the best resources for healing. Listen to the birds, notice the trees, feel the wind, and appreciate the changes in the weather.
Spend time with a pet.
From companionship to unconditional love, pets bring huge benefit to our lives. Dogs, cats, and horses especially can reduce anxiety, stress, and lower blood pressure. Often, pets are empathetic to our moods and can tell when we are not feeling well. They are called our ‘best friend’ for a reason!
Prioritize getting organized.
Declutter the things in your mind by writing them in a planner or calendar. Keep a running grocery list or to-do list so you never again have to stress about what you may be forgetting. (Just don’t forget the list!). Another quick organizational habit is to prepare keys, purses, backpacks, briefcases, and coats to be ready to go for the next morning. This gives your mind more room to be creative!
Prepare your own meals.
Make this an event. Cook. Fast food and pre-made meals lack sufficient nutrients and are often more calorie-dense than fresh meals made at home. Even if it’s once a week, try cooking a healthy meal. The recent rise in meal kits and meal delivery services may help you get started.
Read a book on self-care.
Instead of scrolling a news feed for entertainment, try reading a self-help or self-care book. This can help you slow down, improve your mood, and help you be mindful and present where you are. Listen to a podcast on resilience, self-care, and the science of self-care practices.
Schedule daily self-care time like an important appointment.
You wouldn’t cancel breakfast with your favorite author, would you? Then why are we so quick to sweep our self-care aside? Self-care can help you stay grounded and keep goals at the forefront of your mind. Start small. Wake up 15 minutes early to have a cup of delicious herbal or green tea and practice deep breathing. Or take a walk around the block on your lunch break. The more you practice incorporating self-care into your schedule, the better you can grow and prioritize the things most important to you. Aim to take 5 minutes 5 times a day to practice self-care. 5 X 5. It’s like rebooting your brain for better health and performance.
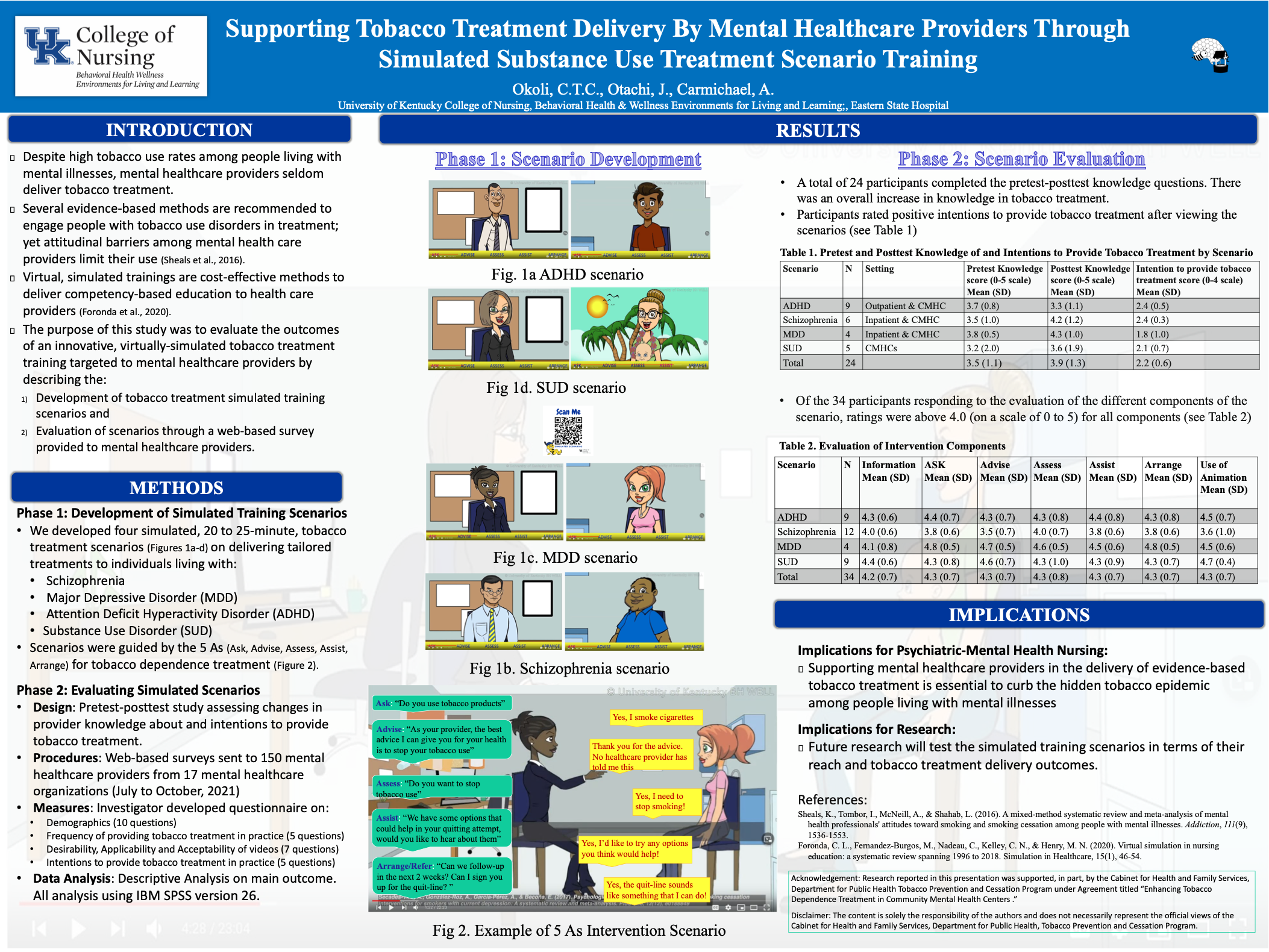
People with mental illness (MI) have a disproportionate tobacco-related disease burden and mortality. Tobacco-use rates in people with MI are nearly twice that of the general population. Reasons for tobacco-use in this population may be a result of diminished tobacco-related disease risk perceptions. The purpose of this study was to examine the reasons for tobacco-use and perceived tobacco-related health risks among psychiatric inpatients. A correlational design was employed to survey a convenient sample of 137 patients from a psychiatric facility in central Kentucky. Information obtained from participants included demographics, psychiatric diagnoses, tobacco-use and exposure history, medical illness history, reasons for tobacco-use, and tobacco-related illness risk perceptions. The primary reasons participants endorsed for tobacco-use were for stress reduction, followed by addiction, then boredom, psychiatric symptom control, social, and negative mood. In addition, about 72% of participants used tobacco to cope with MI symptoms and 52% to manage the side effects of their medications. Participants were most likely to endorse that tobacco-use caused lung disease (83.2%), heart disease (79.6%), cancer (77.4%), and premature mortality (79.6%) but were less likely to admit that it may cause addiction to other drugs (39.4%) or MI (23.4%). Given the high endorsement of tobacco-use for stress reduction and psychiatric symptom control, it is important for mental health nurses to properly educate consumers on tobacco addiction and evidence of its effects on mental health. Strategies to incorporate our study findings into routine mental health services may address the tobacco-use disparities experienced by people with MI.
Obsessive-Compulsive Disorder (OCD) is characterized by obsessions and recurring compulsions. Obsessions are persisting, uninvited, unwanted, and anxiety-provoking thoughts, impulses, or images. In response to obsessions, compulsions ensue as an attempt to reduce distress. Compulsions are repetitive mental acts or behaviors.
Read Transcript
OCD symptoms
4 dimensions of OCD Symptoms:
Concerns about germs and contamination,
Concerns about being responsible for harm, injury, or bad luck,
Unacceptable thoughts, and
Concerns about symmetry, completeness, and the need for things to be “just right.”
It is estimated that 2.3% of adults in the U.S. will experience OCD at some point in their lifetime with females being more likely to experience it. That sounds like a small percentage. So why does this deserve attention? Because over half of people living with OCD have serious impairment in daily functioning. As an example, someone with OCD may have obsessive thoughts that there are germs on their hands. Further impairment would have them fearful of becoming sick because of potential germs on their hands. For those with serious impairment, it moves beyond obsessions to compulsions of washing their hands an excessive number of times per day to reduce their stress about becoming sick. This example portrays the importance of identifying symptoms early and providing effective treatments.
Treatment Options
Treatments such as cognitive behavior therapy (CBT) and medication can help. Yet over half of the people treated are shown to relapse. However, there is hope because mindfulness has been shown to be effective in reducing residual symptoms that CBT may not address.
Mindfulness is a heightened awareness of and attention to an incident or existing reality. In addition, with greater mindfulness comes attitudes of acceptance, openness, and curiosity. These improvements in attitude can help reduce OCD symptoms because it can serve as a coping mechanism and separate the person from their obsessions and compulsions. These positive changes in thought help with “letting go” of obsessions which, in turn, decrease symptoms. Even though mindfulness is consistently shown in studies to reduce OCD symptoms, it is not widely used and is considered a “third wave” treatment after CBT and medication. Part of the reason it is a lesser-used treatment may be because more needs to be understood about which facets of mindfulness may attribute to improved OCD symptoms.
Mindfulness
The facets of mindfulness include non-react, observe, act aware, describe, and non-judge:
Non-react refers to one’s ability to notice but not react to feelings, emotions, and situations.
Observe refers to one’s ability to pay attention to or notice their thoughts, feelings, perceptions, and sensations.
Act aware refers to one’s ability to be aware, concentrate, not get distracted, and not “run on autopilot.”
Describe refers to one’s ability to explain and label their feelings, beliefs, opinions, expectations, and thoughts.
And lastly, non-judge refers to one’s ability to view their thoughts, perceptions, feelings, and situations without judgment.
One study found that compared to a group of people living without OCD, people living with OCD scored much lower in the mindfulness facets of describe, act aware, and non-judge, but did not differ in the mindfulness facets of observe and non-react. Not only does this allow health professionals insight as to who might be more likely to experience debilitating OCD symptoms but also it narrows down the focus of treatment to the three facets of mindfulness most impacted by OCD.
One reason I want to go into occupational therapy is to help advance work in this field so that we can support people living with OCD to live the life they want to live.
References
Abramowitz J.S., Reuman L. (2020) Obsessive Compulsive Disorder. In: Zeigler-Hill V., Shackelford T.K. (eds) Encyclopedia of Personality and Individual Differences. Springer, Cham. https://doi.org/10.1007/978-3-319-24612-3_919
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment (Odessa, Fla.), 13(1), 27-45. https://doi.org/10.1177/1073191105283504
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., . . . Devins, G. (2006). Mindfulness: A Proposed Operational Definition. Clinical Psychology (New York, N.Y.), 11(3), 230-241. https://doi.org/10.1093/clipsy/bph077
Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric Properties of the Five Facet Mindfulness Questionnaire in Depressed Adults and Development of a Short Form. Assessment (Odessa, Fla.), 18(3), 308-320. https://doi.org/10.1177/1073191111408231
Brown, K. W., & Ryan, R. M. (2003). The Benefits of Being Present. Journal of Personality and Social Psychology, 84(4), 822-848. https://doi.org/10.1037/0022-3514.84.4.822
Crowe, K., & McKay, D. (2016). Mindfulness, Obsessive-Compulsive Symptoms, and Executive Dysfunction. Cognitive Therapy and Research, 40(5), 627-644. https://doi.org/10.1007/s10608-016-9777-x
Hale, L., Strauss, C., & Taylor, B. L. (2013). The effectiveness and acceptability of mindfulness‐based therapy for obsessive compulsive disorder: A review of the literature. Mindfulness, 4(4), 375–382. https://doi.org/10.1007/s12671-012-0137-y
Hanstede, M., Gidron, Y., & Nyklíček, I. (2008). The Effects of a Mindfulness Intervention on Obsessive-Compulsive Symptoms in a Non-Clinical Student Population. The Journal of Nervous and Mental Disease, 196(10), 776-779. https://doi.org/10.1097/NMD.0b013e31818786b8
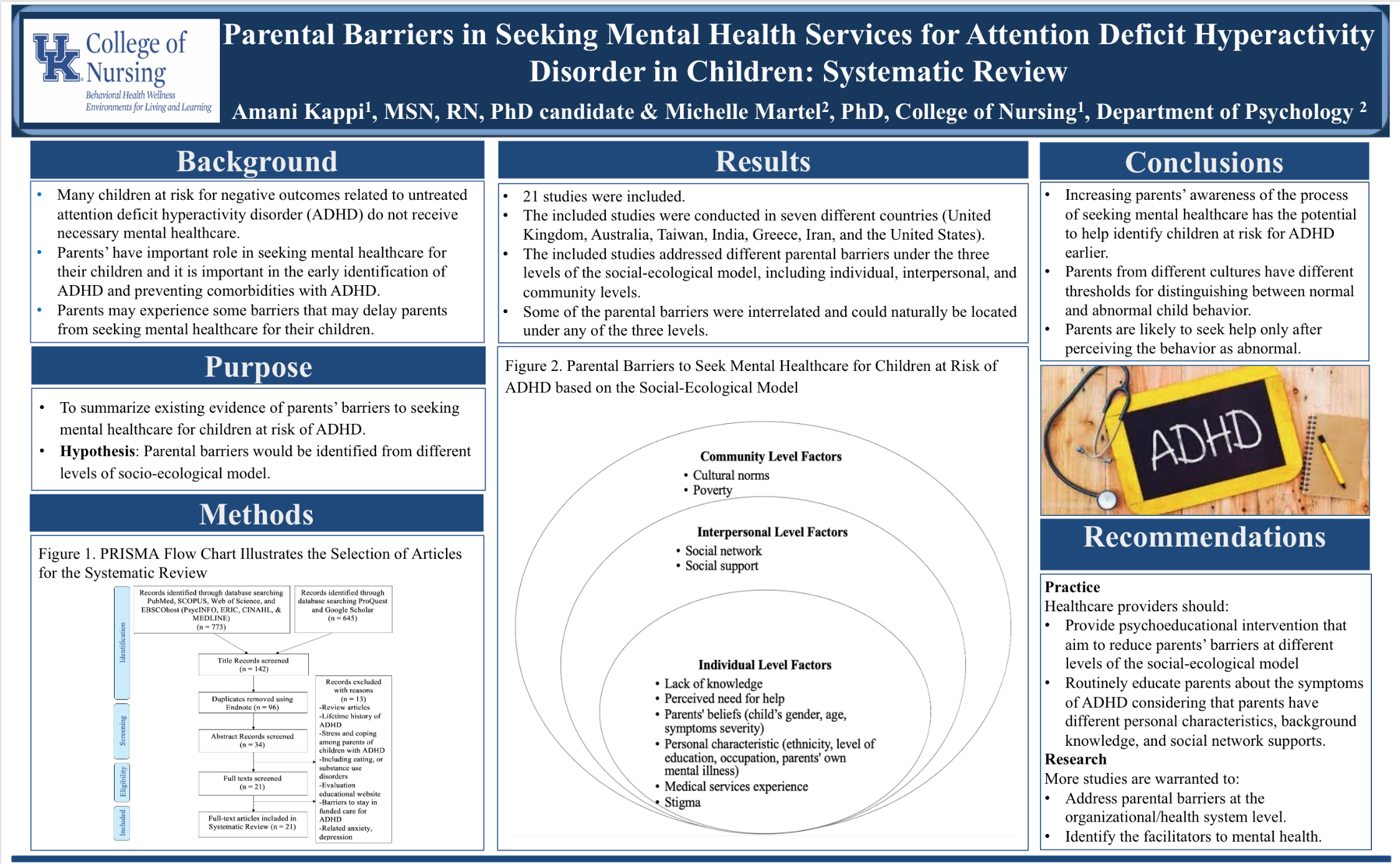
Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood neurodevelopmental diseases and nearly two thirds of children with ADHD have symptoms that persist into adulthood. Approximately 750,000 children with special health care needs transition from pediatric to adult health care annually in the United States. For youth with ADHD, organized, coordinated, and systematic care transition from pediatric to adult health care providers is essential to prevent negative consequences related to unmanaged ADHD symptoms and to optimize health and promote maximum functioning. The Got Transition model’s 6 core elements provide a guide to support successful transition for adolescents with ADHD.,
Evidence based practice starts with a question. When we have a question in mind, we look up the research on the topic and evaluate it to see what the outcomes are. It is important to evaluate current programs and materials in order to ensure that healthcare professionals are doing evidence based and effective work. Evidence based practice is really important because it questions if we can improve upon what we are doing so we can better our treatment and the well-being of our patients.
Motivational interviewing is a way for the clinician and client to talk about the clients reasons for change. The clinician helps the client understand reasons for change and helps elicit the clients desire for change. It has been effectively used for addiction behaviors, tobacco treatment, weight loss interventions, and other situations where an individual wants to change their negative health behaviors. The approach expresses empathy, avoids arguing, develops discrepancy, and supports self-efficacy. It is useful in clinical situations where ambivalence is high, desire is low, motivation is low, and confidence is low. The main takeaway of motivational interviewing is to understand that there is no information that is new to the client (I.e. they know the substance is harmful) and the doctor gently helps the client understand that they are an expert in their own health and any previous experience trying to quit. The approach is a team effort of both the clinician and client.
Transcript
Chloe: Hi and welcome to the BH WELL video blog. I'm Chloe Robertson, your host. BH WELL stands for Behavioral Health Wellness Environments for Living and Learning. Today on the vlog we have with us Dr. Lovoria Williams he is an associate professor at the University of Kentucky College of Nursing. She's here with us to discuss motivational interviewing. Hi Dr. Williams.
Dr. Williams: Hi, how are you today?
Chloe: Good how're you?
Dr. Williams: Good.
What is motivational interviewing?
Dr. Williams: Wow, that's a big question for such a complex style of conversation. But simply, motivational interviewing is a way for the clinician and the client communicate to one another in a way where the clinician helps the client explore their reasons for change. The client is the expert and the clinician is also the expert, but it's where the clinician helps the client understand reasons for change and helps elicit from the client reasons why they should be motivated to change.
In what areas has motivational interviewing been used effectively?
Dr. Williams: Motivational interviewing has been used effectively in many areas. It's been used in addiction behaviors for tobacco treatment. It's been used in weight loss interventions. It's been used in any situation where an individual wants to change their behaviors or the clinician believes that what the individuals doing may affect their health in a negative way and they want to guide the individual to change their behaviors.
In what clinical situations is motivational interviewing most useful?
Dr. Williams: Any clinical situation where ambivalence is high, desire is low, motivation is low, and confidence is low. So that could be in the case of tobacco, the individual uses tobacco and the clinician is trying to have a conversation with the individual about changing their tobacco use behaviors. The individual may be ambivalent because tobacco helps them, and helps them when they’re stressed, or it helps them calm down and so their ambivalent. They know the information about the ill health effects, but they still are ambivalent about changing their behavior. Or, again in the case of tobacco, they may have tried before so their confidence is low because they perhaps have tried unsuccessfully before; And their motivation could also be low because again they desire it; And then their desire may be low because they have some pleasure from using tobacco. So it’s most effective in the clinical situation where those four factors exist.
For more in depth information on Motivational Interviewing, check out the book Motivational Interviewing: Helping People Change by Miller & Rollnick. ISBN 9781609182274
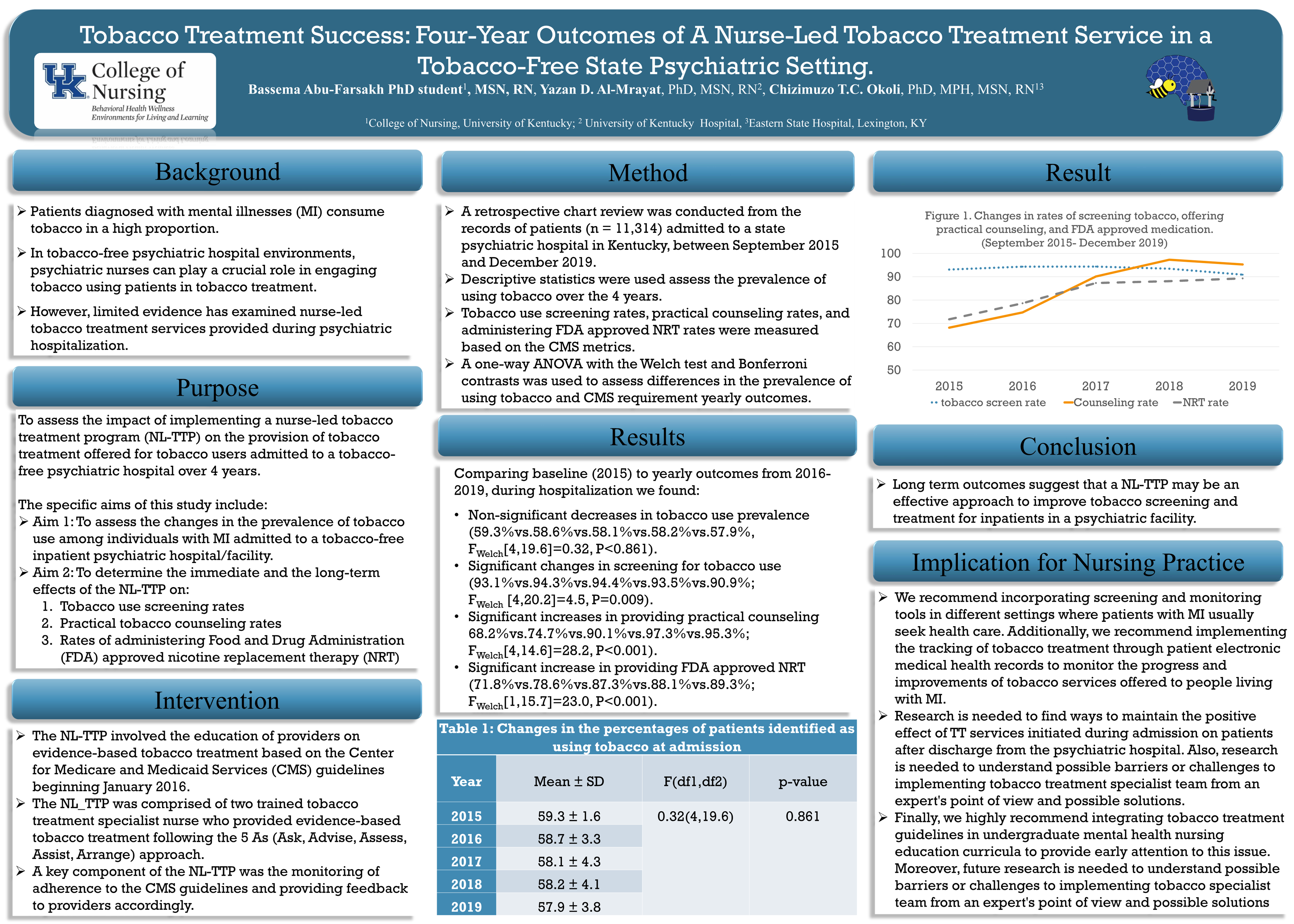
A nurse-led tobacco treatment program (NL-TTP) was implemented on the provision of tobacco treatment offered for tobacco users admitted to a tobacco-free psychiatric hospital over 4 years. Results include non-significant decreases in tobacco use, significant changes in tobacco screening, significant increases in provided practical counseling, and significant increase in providing FDA approved NRT. Long term outcomes suggest NL-TTP to be an affective approach to improve tobacco screening and treatment for psychiatric facility inpatients.